

Liberal transfusion strategy to prevent mortality and anaemia-associated, ischaemic events in elderly non-cardiac surgical patients - the study design of the LIBERAL-Trial
- PMID: 30717805
- PMCID: PMC6360712
- DOI: 10.1186/s13063-019-3200-3
Liberal transfusion strategy to prevent mortality and anaemia-associated, ischaemic events in elderly non-cardiac surgical patients - the study design of the LIBERAL-Trial
Abstract
Background: Perioperative anaemia leads to impaired oxygen supply with a risk of vital organ ischaemia. In healthy and fit individuals, anaemia can be compensated by several mechanisms. Elderly patients, however, have less compensatory mechanisms because of multiple co-morbidities and age-related decline of functional reserves. The purpose of the study is to evaluate whether elderly surgical patients may benefit from a liberal red blood cell (RBC) transfusion strategy compared to a restrictive transfusion strategy.
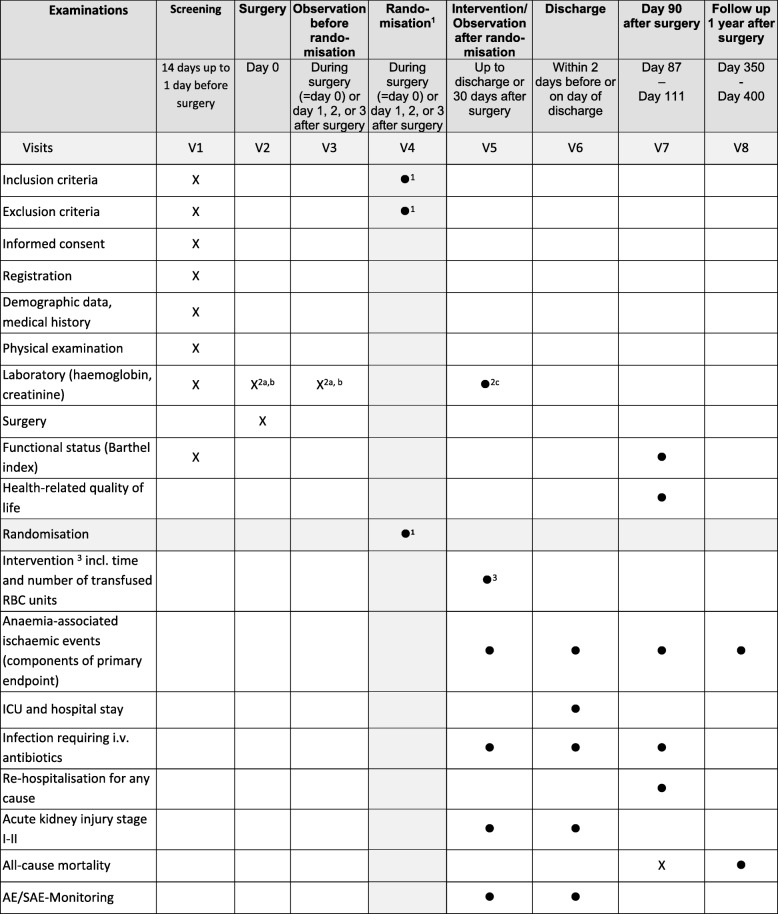
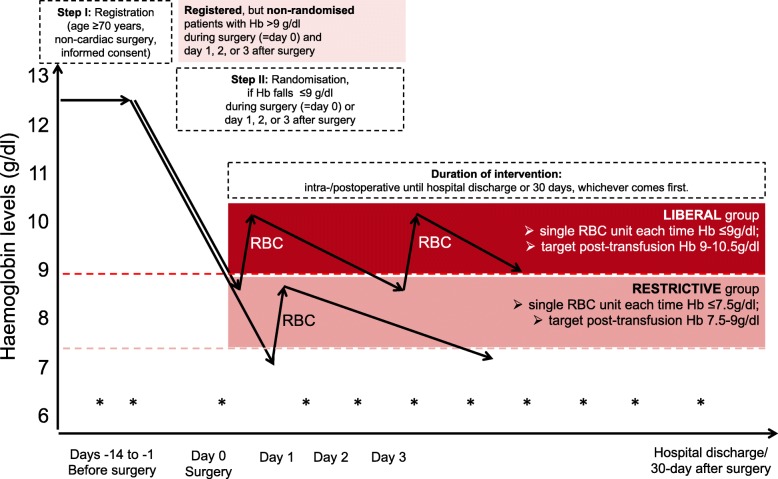
Methods: The LIBERAL Trial is a prospective, randomized, multicentre, controlled clinical phase IV trial randomising 2470 elderly (≥ 70 years) patients undergoing intermediate- or high-risk non-cardiac surgery. Registered patients will be randomised only if Haemoglobin (Hb) reaches ≤9 g/dl during surgery or within 3 days after surgery either to the LIBERAL group (transfusion of a single RBC unit when Hb ≤ 9 g/dl with a target range for the post-transfusion Hb level of 9-10.5 g/dl) or the RESTRICTIVE group (transfusion of a single RBC unit when Hb ≤ 7.5 g/dl with a target range for the post-transfusion Hb level of 7.5-9 g/dl). The intervention per patient will be followed until hospital discharge or up to 30 days after surgery, whichever occurs first. The primary efficacy outcome is defined as a composite of all-cause mortality, acute myocardial infarction, acute ischaemic stroke, acute kidney injury (stage III), acute mesenteric ischaemia and acute peripheral vascular ischaemia within 90 days after surgery. Infections requiring iv antibiotics with re-hospitalisation are assessed as important secondary endpoint. The primary endpoint will be analysed by logistic regression adjusting for age, cancer surgery (y/n), type of surgery (intermediate- or high-risk), and incorporating centres as random effect.
Discussion: The LIBERAL-Trial will evaluate whether a liberal transfusion strategy reduces the occurrence of major adverse events after non-cardiac surgery in the geriatric population compared to a restrictive strategy within 90 days after surgery.
Trial registration: ClinicalTrials.gov (identifier: NCT03369210 ).
Keywords: Red blood cell transfusion; anaemia; elderly patients; surgery.
Conflict of interest statement
Ethics approval and consent to participate
Study protocol V3.0 (EudraCT-Nr 2016–004446-29), patient information, and informed consent were approved by the Ethics Committee of the University of Frankfurt (Ref: 139/17F) and of all participating centres. At the same time the study documents have been approved by the responsible federal authority (Paul-Ehrlich-Institute) according to the requirements of GCP-V § 7. Each patient must give written informed consent to participate in the study.
Consent for publication
Not applicable.
Competing interests
M.M and E.S. work for the German Red Cross, deliver RBC units and may have a financial competing interest. All other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Hebert PC, Wells G, Blajchman MA, Marshall J, Martin C, Pagliarello G, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med. 1999;340:409–417. doi: 10.1056/NEJM199902113400601. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
