

Independent Left Ventricular Morphometric Atlases Show Consistent Relationships with Cardiovascular Risk Factors: A UK Biobank Study
- PMID: 30718635
- PMCID: PMC6362245
- DOI: 10.1038/s41598-018-37916-6
Independent Left Ventricular Morphometric Atlases Show Consistent Relationships with Cardiovascular Risk Factors: A UK Biobank Study
Abstract
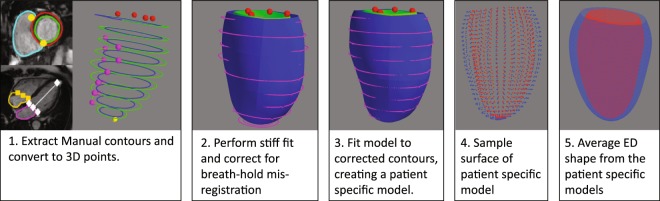
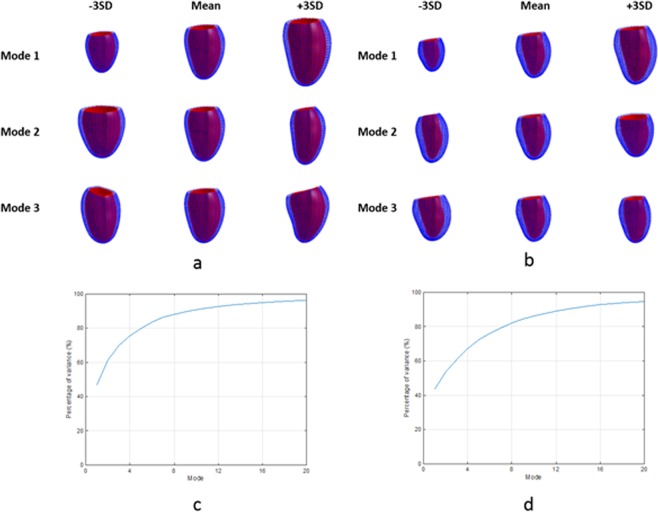
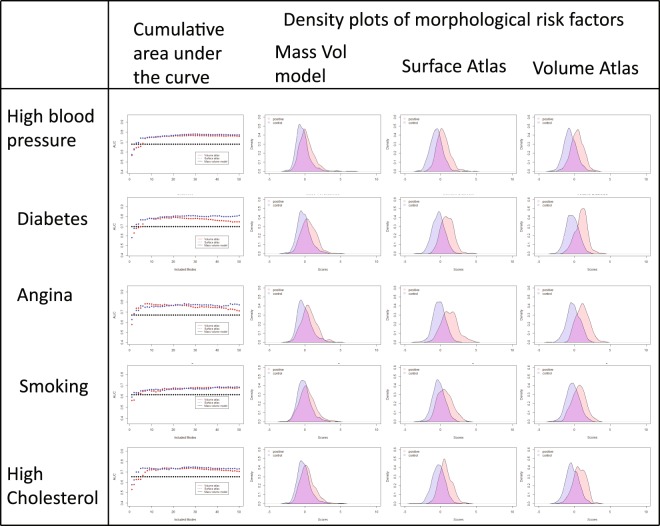
Left ventricular (LV) mass and volume are important indicators of clinical and pre-clinical disease processes. However, much of the shape information present in modern imaging examinations is currently ignored. Morphometric atlases enable precise quantification of shape and function, but there has been no objective comparison of different atlases in the same cohort. We compared two independent LV atlases using MRI scans of 4547 UK Biobank participants: (i) a volume atlas derived by automatic non-rigid registration of image volumes to a common template, and (ii) a surface atlas derived from manually drawn epicardial and endocardial surface contours. The strength of associations between atlas principal components and cardiovascular risk factors (smoking, diabetes, high blood pressure, high cholesterol and angina) were quantified with logistic regression models and five-fold cross validation, using area under the ROC curve (AUC) and Akaike Information Criterion (AIC) metrics. Both atlases exhibited similar principal components, showed similar relationships with risk factors, and had stronger associations (higher AUC and lower AIC) than a reference model based on LV mass and volume, for all risk factors (DeLong p < 0.05). Morphometric variations associated with each risk factor could be quantified and visualized and were similar between atlases. UK Biobank LV shape atlases are robust to construction method and show stronger relationships with cardiovascular risk factors than mass and volume.
Conflict of interest statement
S.E.P. provides consultancy to Circle Cardiovascular Imaging Inc, Calgary, Canada. A.Y. provides consultancy to Siemens Healthineers, Erlangen, Germany.
Figures



References
-
- Wong, S. P. et al. Relation of left ventricular sphericity to 10-year survival after acute myocardial infarction. Am J Cardiol94, 1270–1275, doi:S0002-9149(04)01224-X (2004). - PubMed
