

High percentages and activity of synovial fluid NK cells present in patients with advanced stage active Rheumatoid Arthritis
- PMID: 30718650
- PMCID: PMC6361912
- DOI: 10.1038/s41598-018-37448-z
High percentages and activity of synovial fluid NK cells present in patients with advanced stage active Rheumatoid Arthritis
Abstract
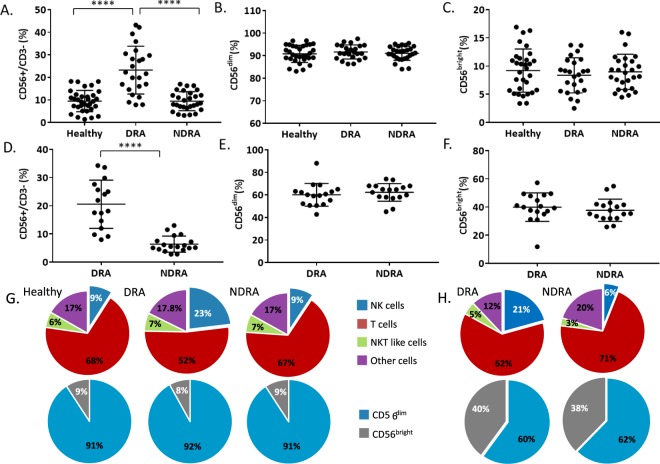
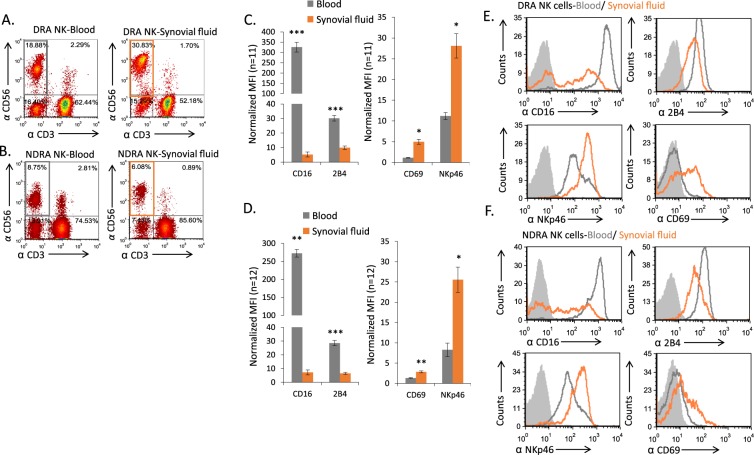
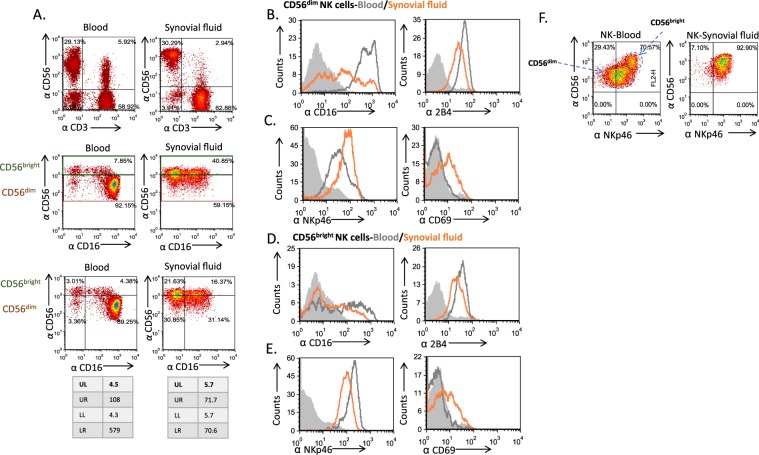
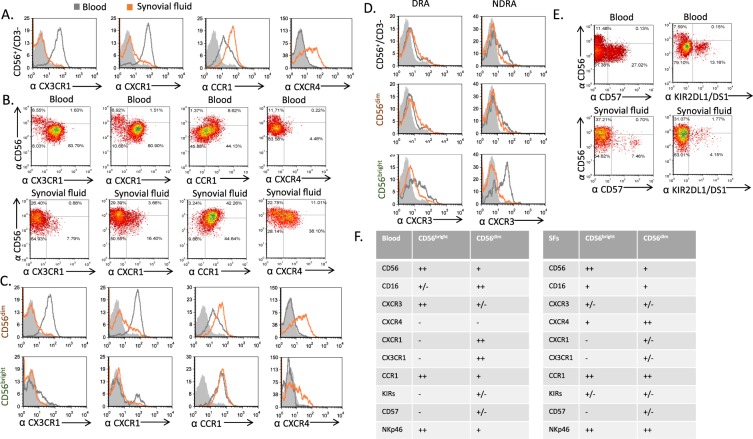
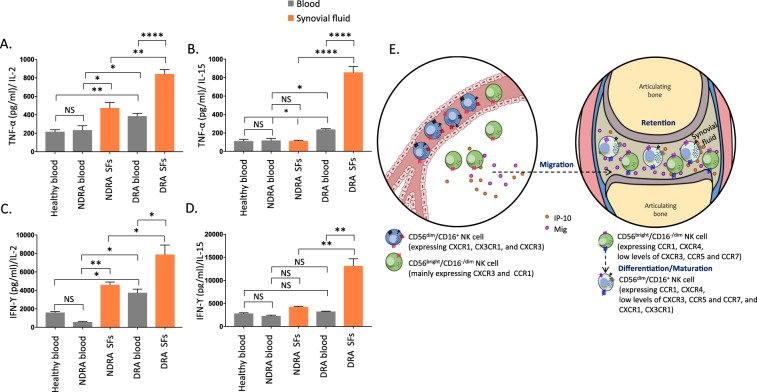
Rheumatoid Arthritis (RA) causes chronic inflammation of joints. The cytokines TNFα and IFNγ are central players in RA, however their source has not been fully elucidated. Natural Killer (NK) cells are best known for their role in elimination of viral-infected and transformed cells, and they secrete pro-inflammatory cytokines. NK cells are present in the synovial fluids (SFs) of RA patients and are considered to be important in bone destruction. However, the phenotype and function of NK cells in the SFs of patients with erosive deformative RA (DRA) versus non-deformative RA (NDRA) is poorly characterized. Here we characterize the NK cell populations present in the blood and SFs of DRA and NDRA patients. We demonstrate that a distinct population of activated synovial fluid NK (sfNK) cells constitutes a large proportion of immune cells found in the SFs of DRA patients. We discovered that although sfNK cells in both DRA and NDRA patients have similar phenotypes, they function differently. The DRA sfNK secrete more TNFα and IFNγ upon exposure to IL-2 and IL-15. Consequently, we suggest that sfNK cells may be a marker for more severely destructive RA disease.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Shah, A. & Clair, E. W. St. Rheumatoid Arthritis. In Harrison’s Principles of Internal Medicine, 19e (eds Kasper, D. et al.) (McGraw-Hill Education, New York, NY, 2015).
-
- Cope AP, Schulze-Koops H, Aringer M. The central role of T cells in rheumatoid arthritis. Clin Exp Rheumatol. 2007;25:S4–11. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
