

High-resolution fingerprinting of Candida parapsilosis isolates suggests persistence and transmission of infections among neonatal intensive care unit patients in Kuwait
- PMID: 30718894
- PMCID: PMC6361955
- DOI: 10.1038/s41598-018-37855-2
High-resolution fingerprinting of Candida parapsilosis isolates suggests persistence and transmission of infections among neonatal intensive care unit patients in Kuwait
Abstract
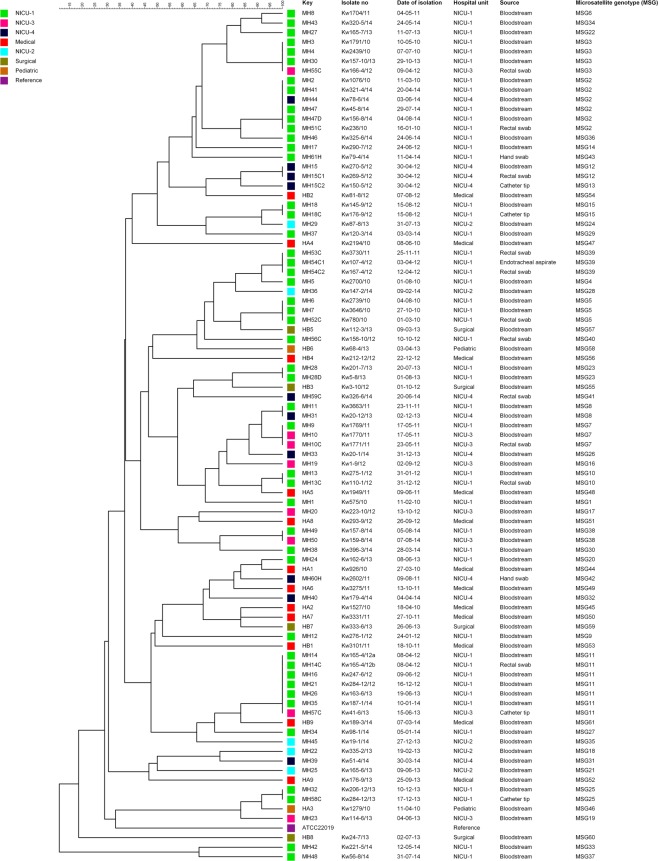
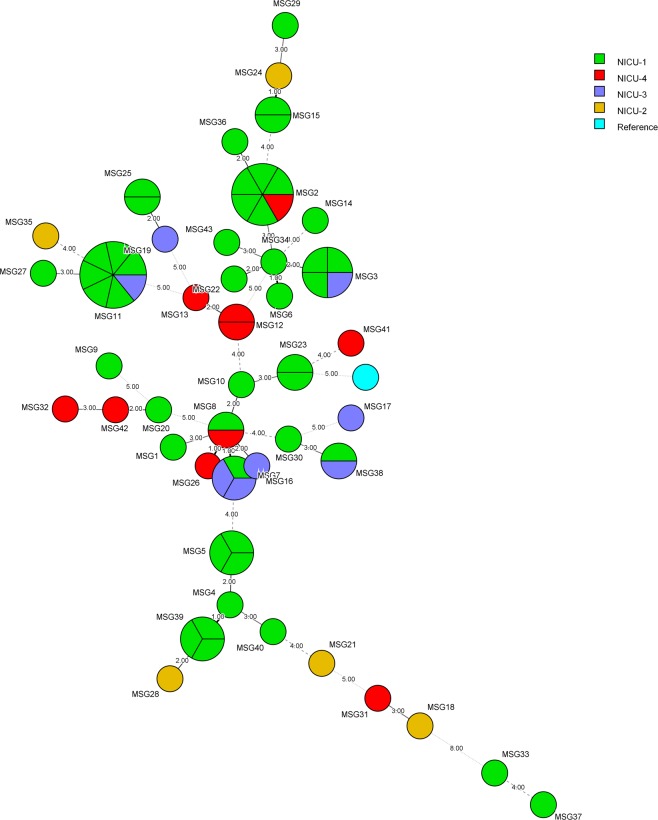
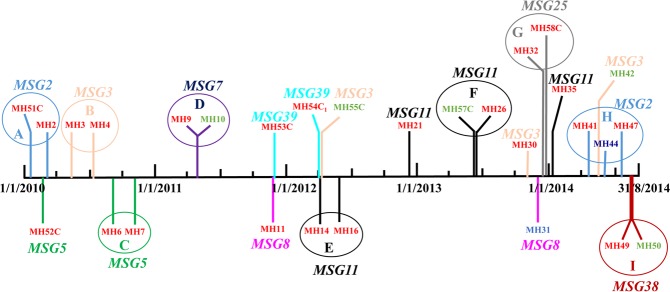
Candida parapsilosis causes ~35% of all candidemia cases in neonates. High-resolution fingerprinting of C. parapsilosis isolates from neonatal intensive care unit (NICU) patients in Maternity Hospital (MH) was performed to identify epidemiologically related strains. Sixty-eight bloodstream/colonizing strains isolated from 59 NICU patients, two isolates from health care workers (HCWs) from MH and 18 bloodstream isolates from two other hospitals were used. Six microsatellite markers were employed, isolates were assigned a numerical microsatellite genotype (MSG), dendrogram was constructed and similarities between genotypes were visualized by minimum spanning tree. Fifty bloodstream isolates from MH yielded 37 MSGs with 20 isolates clustering in 7 MSGs. Duplicate isolates and colonizing strains yielded same/highly similar MSG as bloodstream isolates. Colonizing strains from two non-candidemia patients yielded unique MSGs while others belonged to a cluster. All isolates from HCWs and from two other hospitals belonged to unique MSGs. Cluster isolates came from patients in NICU-1 or from neonates in NICU-1 and other NICUs. Clonal complexes comprising closely related genotypes indicative of microevolution were also detected. Our data show that some C. parapsilosis strains have persisted in MH environment over several years and these endemic genotypes were transmitted to other patients in NICU-1 and/or other nearby NICUs.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
