

Patient-Specific Phantomless Estimation of Bone Mineral Density and Its Effects on Finite Element Analysis Results: A Feasibility Study
- PMID: 30719069
- PMCID: PMC6335860
- DOI: 10.1155/2019/4102410
Patient-Specific Phantomless Estimation of Bone Mineral Density and Its Effects on Finite Element Analysis Results: A Feasibility Study
Abstract
Objectives: This study proposes a regression model for the phantomless Hounsfield units (HU) to bone mineral density (BMD) conversion including patient physical factors and analyzes the accuracy of the estimated BMD values.
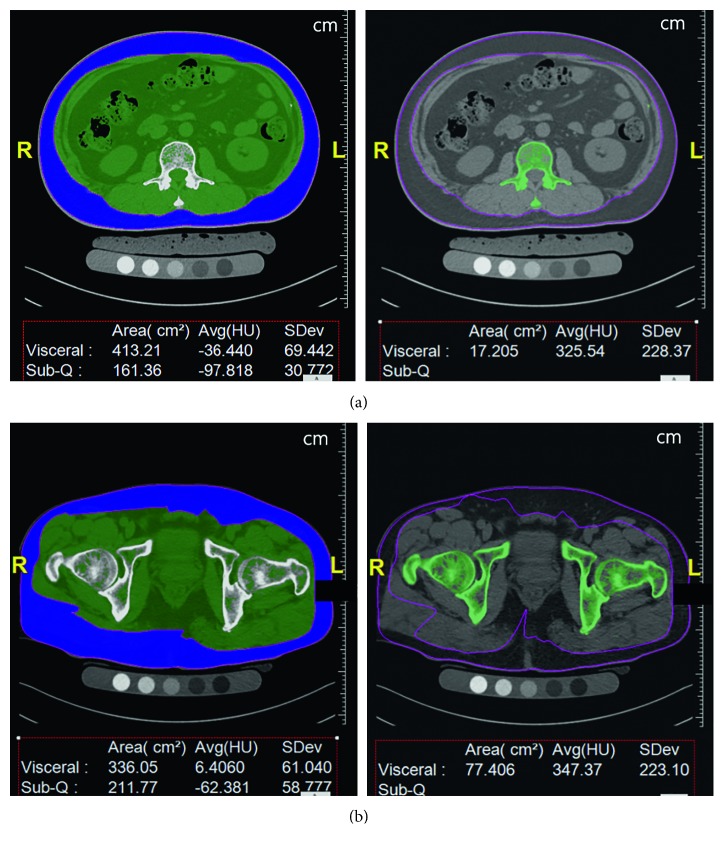
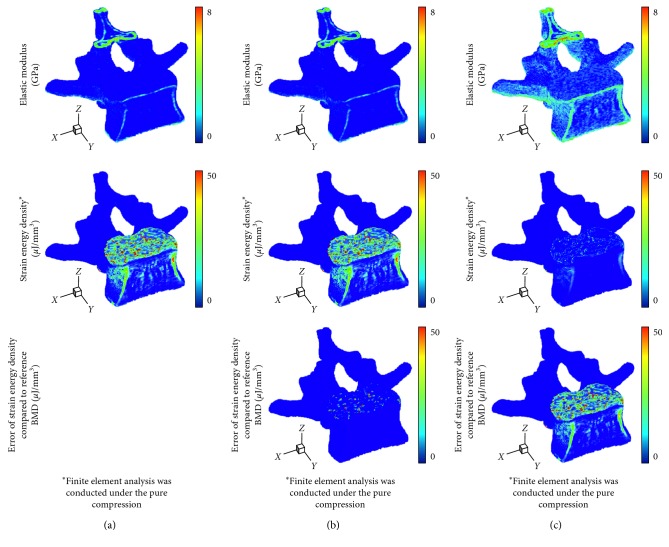
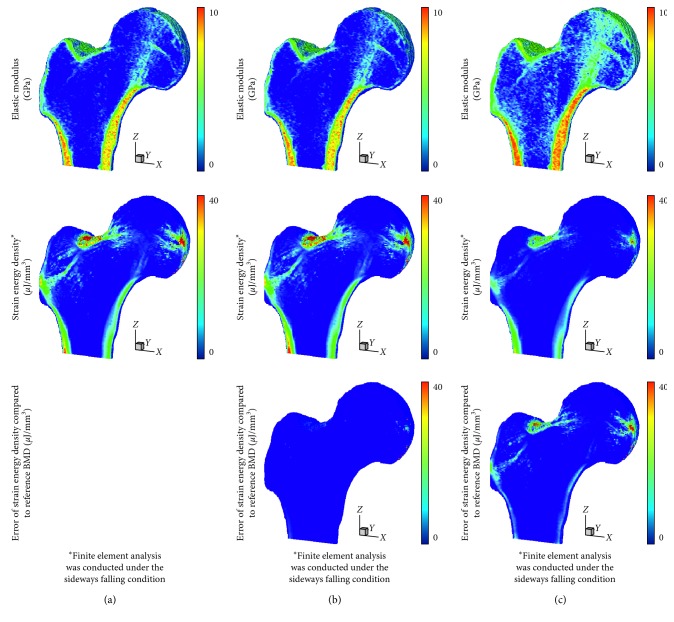
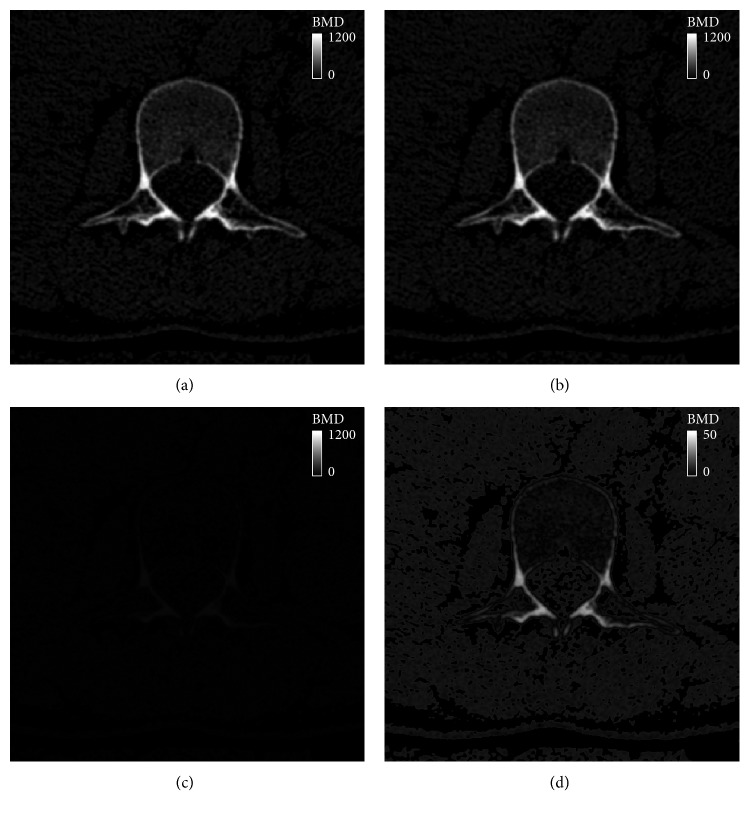
Methods: The HU values, BMDs, circumferences of the body, and cross-sectional areas of bone were measured from 39 quantitative computed tomography images of L2 vertebrae and hips. Then, the phantomless HU-to-BMD conversion was derived using a multiple linear regression model. For the statistical analysis, the correlation between the estimated BMD values and the reference BMD values was evaluated using Pearson's correlation test. Voxelwise BMD and finite element analysis (FEA) results were analyzed in terms of root-mean-square error (RMSE) and strain energy density, respectively.
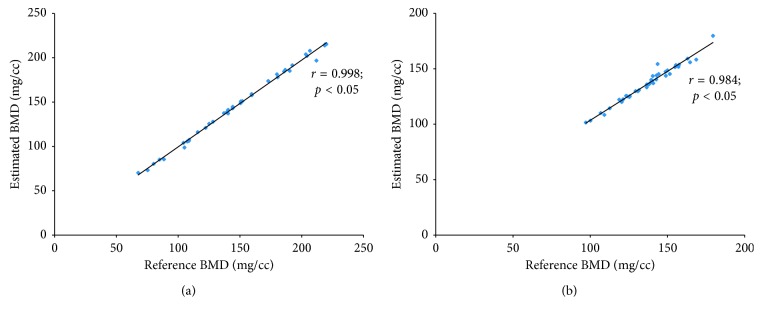
Results: The HU values and circumferences were statistically significant (p < 0.05) for the lumbar spine, whereas only the HU values were statistically significant (p < 0.05) for the proximal femur. The BMD values estimated using the proposed HU-to-BMD conversion were significantly correlated with those measured using the reference phantom: Pearson's correlation coefficients of 0.998 and 0.984 for the lumbar spine and proximal femur, respectively. The RMSEs of the estimated BMD values for the lumbar spine and hip were 4.26 ± 0.60 (mg/cc) and 8.35 ± 0.57 (mg/cc), respectively. The errors of total strain energy were 1.06% and 0.91%, respectively.
Conclusions: The proposed phantomless HU-to-BMD conversion demonstrates the potential of precisely estimating BMD values from CT images without the reference phantom and being utilized as a viable tool for FEA-based quantitative assessment using routine CT images.
Figures

References
-
- Iki M. [Epidemiology of bone and joint disease–the present and future. Epidemiology of osteoporosis and osteoporotic fracture in Japan] Clinical Calcium. 2014;24:657–664. - PubMed
-
- Pereira R. M., Corrente J. E., Chahade W. H., Yoshinari N. H. Evaluation by dual X-ray absorptiometry (DXA) of bone mineral density in children with juvenile chronic arthritis. Clinical and Experimental Rheumatology. 1998;16(4):495–501. - PubMed
-
- Finkelstein J. S., Klibanski A., Neer R. M. Evaluation of lumber spine bone mineral density (BMD) using dual energy x-ray absorptiometry (DXA) in 21 young men with histories of constitutionally-delayed puberty. Journal of Clinical Endocrinology and Metabolism. 1999;84(9):3403–3404. doi: 10.1210/jcem.84.9.6011-2a. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
