

GITR ligation enhances functionality of tumor-infiltrating T cells in hepatocellular carcinoma
- PMID: 30719701
- PMCID: PMC6619339
- DOI: 10.1002/ijc.32181
GITR ligation enhances functionality of tumor-infiltrating T cells in hepatocellular carcinoma
Abstract
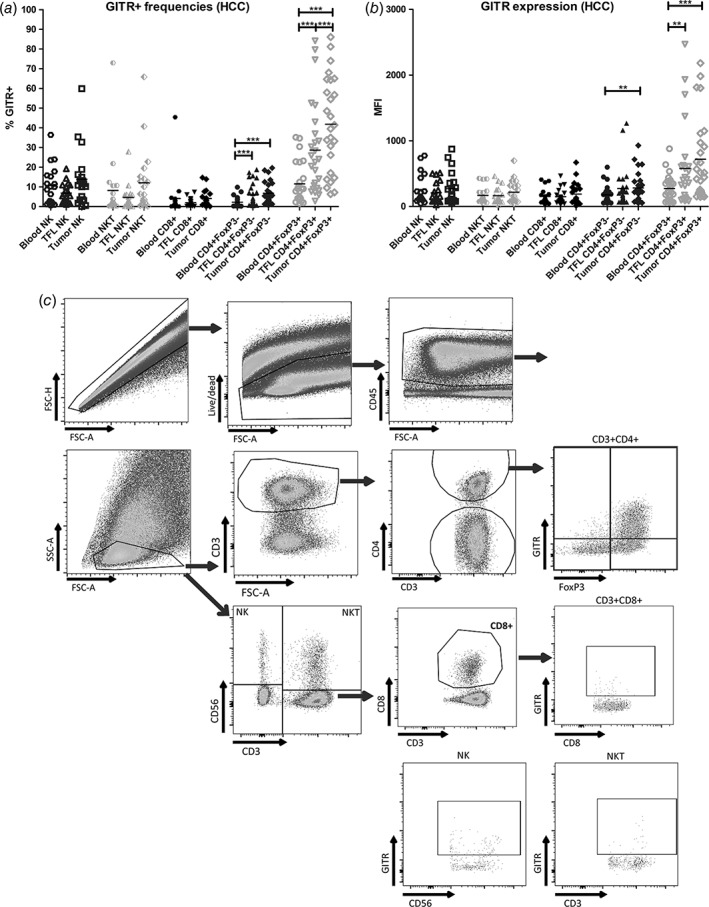
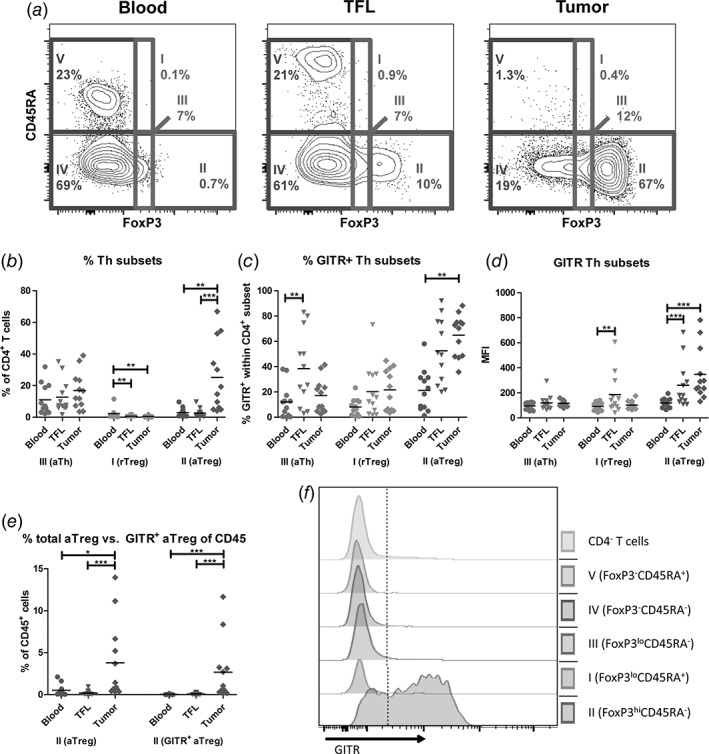
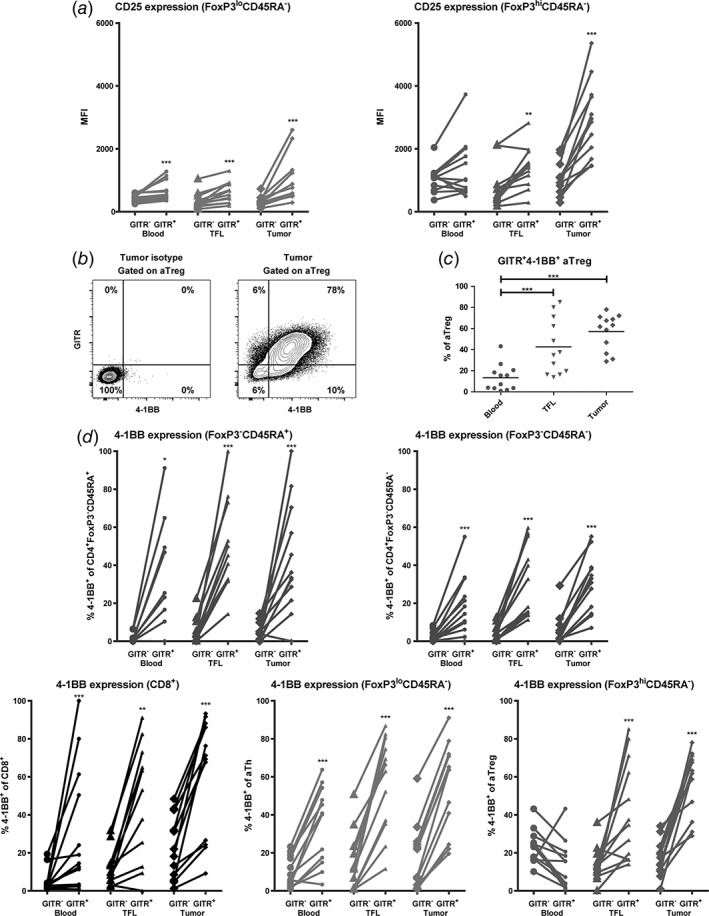
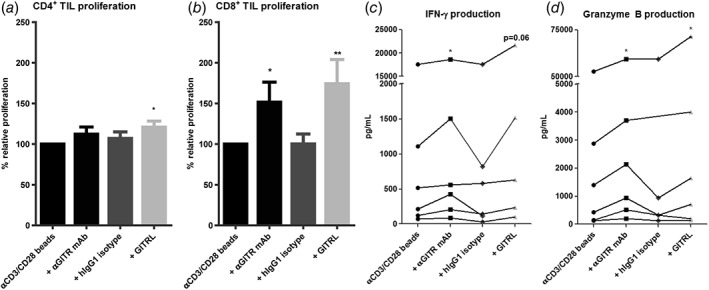
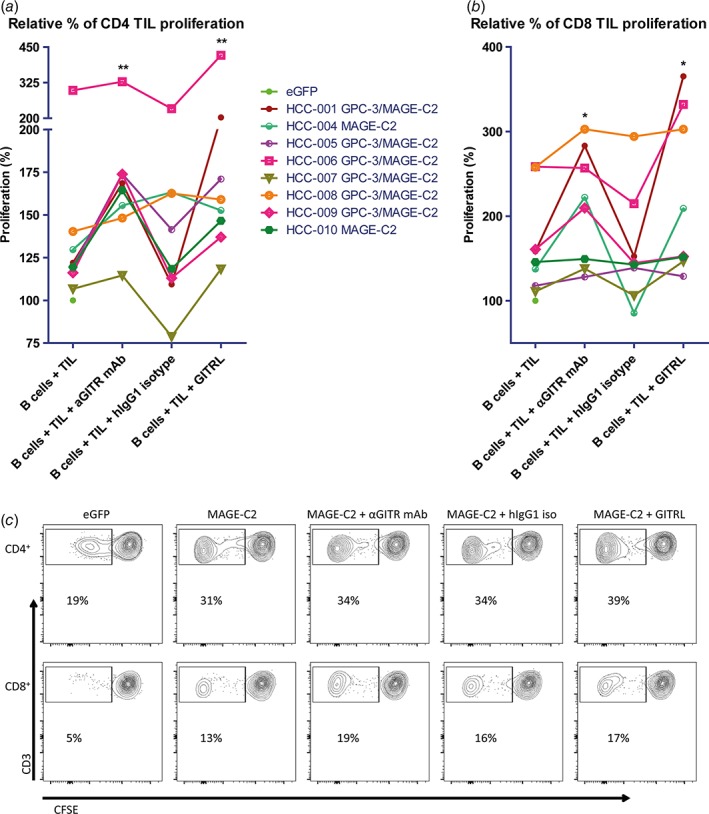
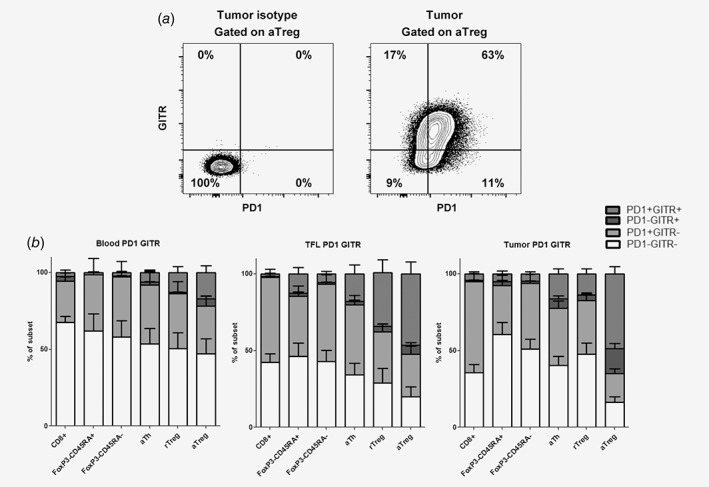
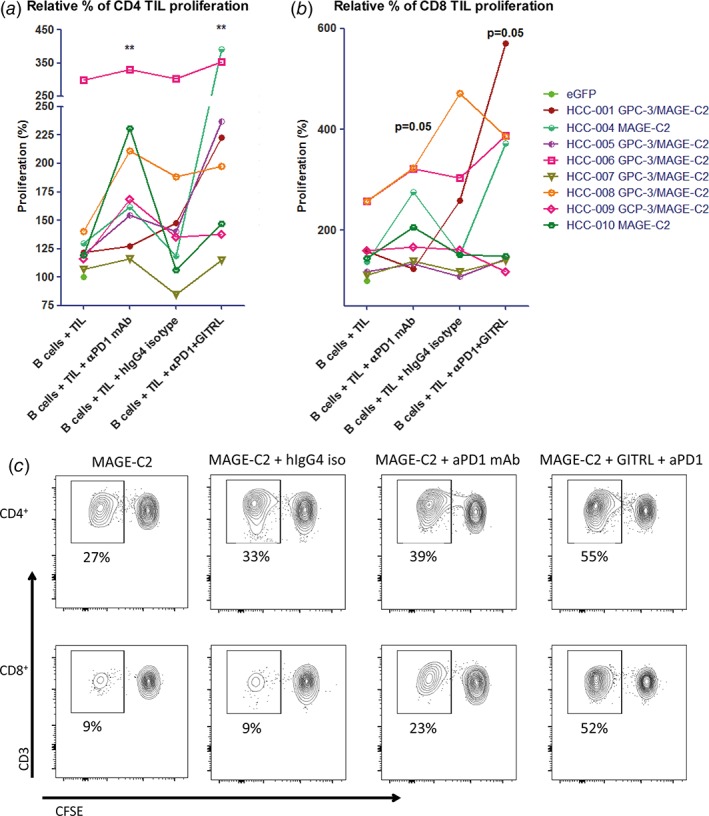
No curative treatment options are available for advanced hepatocellular carcinoma (HCC). Anti-PD1 antibody therapy can induce tumor regression in 20% of advanced HCC patients, demonstrating that co-inhibitory immune checkpoint blockade has therapeutic potential for this type of cancer. However, whether agonistic targeting of co-stimulatory receptors might be able to stimulate anti-tumor immunity in HCC is as yet unknown. We investigated whether agonistic targeting of the co-stimulatory receptor GITR could reinvigorate ex vivo functional responses of tumor-infiltrating lymphocytes (TIL) freshly isolated from resected tumors of HCC patients. In addition, we compared GITR expression between TIL and paired samples of leukocytes isolated from blood and tumor-free liver tissues, and studied the effects of combined GITR and PD1 targeting on ex vivo TIL responses. In all three tissue compartments, CD4+ FoxP3+ regulatory T cells (Treg) showed higher GITR- expression than effector T-cell subsets. The highest expression of GITR was found on CD4+ FoxP3hi CD45RA- activated Treg in tumors. Recombinant GITR-ligand as well as a humanized agonistic anti-GITR antibody enhanced ex vivo proliferative responses of CD4+ and CD8+ TIL to tumor antigens presented by mRNA-transfected autologous B-cell blasts, and also reinforced proliferation, IFN-γ secretion and granzyme B production in stimulations of TIL with CD3/CD28 antibodies. Combining GITR ligation with anti-PD1 antibody nivolumab further enhanced tumor antigen-specific responses of TIL in some, but not all, HCC patients, compared to either single treatment. In conclusion, agonistic targeting of GITR can enhance functionality of HCC TIL, and may therefore be a promising strategy for single or combinatorial immunotherapy in HCC.
Keywords: CD357; GITR; HCC; PD1; TNFRSF18; Treg; cancer immunotherapy.
© 2019 The Authors. International Journal of Cancer published by John Wiley & Sons Ltd on behalf of UICC.
Figures
References
-
- Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin 2015;65:87–108. - PubMed
-
- Mazzanti R, Gramantieri L, Bolondi L. Hepatocellular carcinoma: epidemiology and clinical aspects. Mol Aspects Med 2008;29:130–43. - PubMed
-
- El‐Serag HB, Marrero JA, Rudolph L, et al. Diagnosis and treatment of hepatocellular carcinoma. Gastroenterology 2008;134:1752–63. - PubMed
-
- European Association for the Study of the Liver . EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 2018;69:182–236. - PubMed
-
- Schachter J, Ribas A, Long GV, et al. Pembrolizumab versus ipilimumab for advanced melanoma: final overall survival results of a multicentre, randomised, open‐label phase 3 study (KEYNOTE‐006). Lancet 2017;390:1853–62. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
