

Differences in the distribution of CD20, CD3, CD34 and CD45RO in nasal mucosa and polyps from patients with chronic rhinosinusitis
- PMID: 30720103
- PMCID: PMC6423629
- DOI: 10.3892/mmr.2019.9932
Differences in the distribution of CD20, CD3, CD34 and CD45RO in nasal mucosa and polyps from patients with chronic rhinosinusitis
Abstract
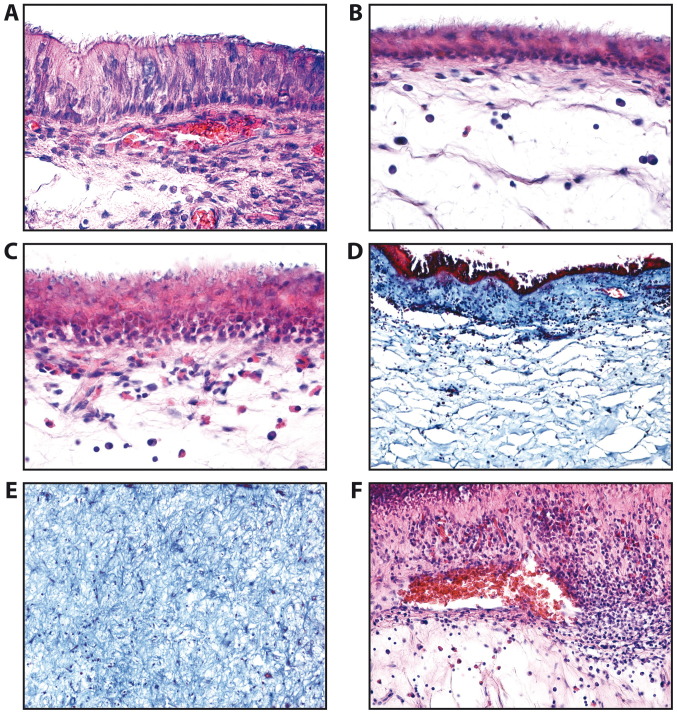
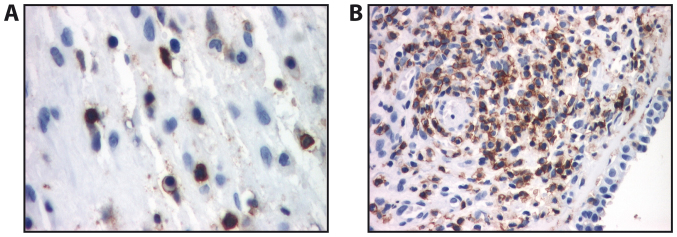
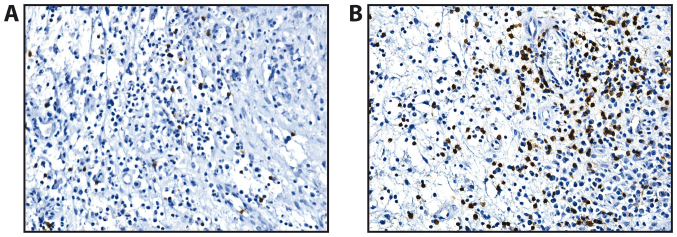
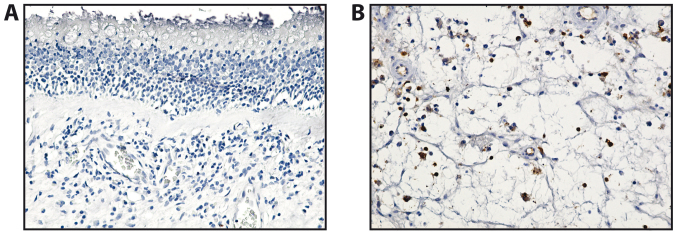
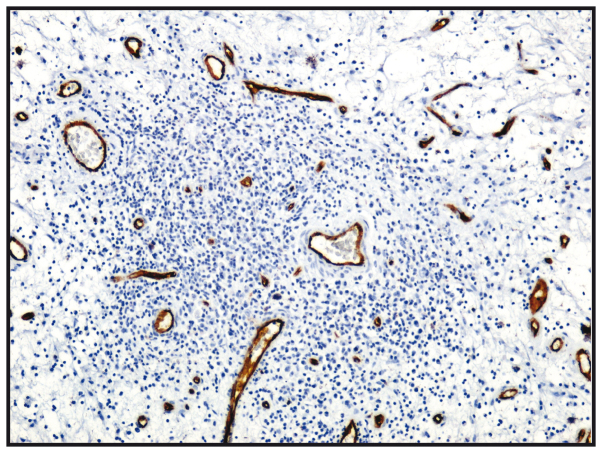
The present study focused on the assessment of the inflammatory infiltrate that characterizes nasal polyps in patients with chronic rhinosinusitis and nasal polyposis. Inflammatory cell type was determined using specific markers. This evaluation was made possible by determining the expression of the following markers: CD20, a marker of B lymphocytes [using activated T cells (ATC) armed with CD20 antibody]; CD3, a marker of T lymphocytes (using ATC armed with anti‑CD3 antibody); CD45, the leukocyte common antigen (using ATC armed with anti‑CD45 antibody; and CD34, for the microvasculature of the nasal polyp (using anti‑CD34 antibody). The diagnosis of chronic rhinosinusitis with nasal polyps (CRSwNP) was made according to current EPOS guidelines based on patient history, clinical examination and nasal endoscopy. We examined surgically resected nasal polyps from 127 patients diagnosed with CRSwNP, who benefited from surgical procedures at the Department of Otorhinolaryngology of our institution. The polyps were analyzed at the Department of Pathology of our institution utilizing histopathological and immunohistochemical methods as follows: Firstly, the tissues were paraffin‑impregnated, sectioned and stained with hematoxylin and eosin. We then examined the expression of CD3, CD20, CD34 and CD45RO by immunohistochemistry with soluble labeled streptavidin biotin (LSAB)/horseradish peroxidase (HRP) complexes. We observed the following histopathological changes: The structure of the epithelium was evidenced by collagenous subjacent stroma with mixed areas, sometimes associated with hyaline zones. In all types of polyps, we also observed a diffuse underlayer or periglandular lymphoplasmacytic in filtrate composed predominantly from T lymphocytes and eosinophils. The histopathological changes suggest the chronic inflammation of the sinus mucosa, which was diffusely distributed in allergic polyps and with nodular distribution in fibro‑inflammatory polyps. The number of B lymphocytes was greater in the fibro‑inflammatory polyps. On the whole, the findings of this study indicate that the inflammatory infiltrate in nasal polyps from patients with CRSwNP is mainly composed of T cells and eosinophils in all types of polyposis. In addition, a diffuse distribution of allergic polyps and the nodular distribution of fibro‑inflammatory polyps, and the hyperplasia of the seromucous glands was observed. The determination of CD20, CD3, CD34 and CD45RO could be used to assess the inflammatory infiltrate of the nasal poplyps in these patients.
Figures
References
-
- Khairuddin NK, Salina H, Gendeh BS, Wan Hamizan AK, Lund VJ. Quality of life and recurrence of disease in patients with eosinophilic and non-eosinophilic 1 chronic rhinosinusitis with nasal polyposis. Med J Malaysia. 2018;73:1–6. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
