

Multicolumn spinal cord stimulation for predominant back pain in failed back surgery syndrome patients: a multicenter randomized controlled trial
- PMID: 30720582
- PMCID: PMC6553955
- DOI: 10.1097/j.pain.0000000000001510
Multicolumn spinal cord stimulation for predominant back pain in failed back surgery syndrome patients: a multicenter randomized controlled trial
Abstract
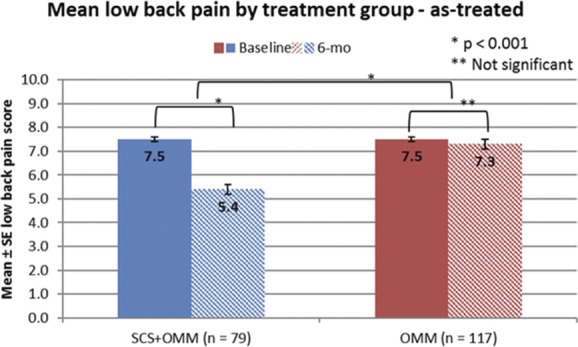
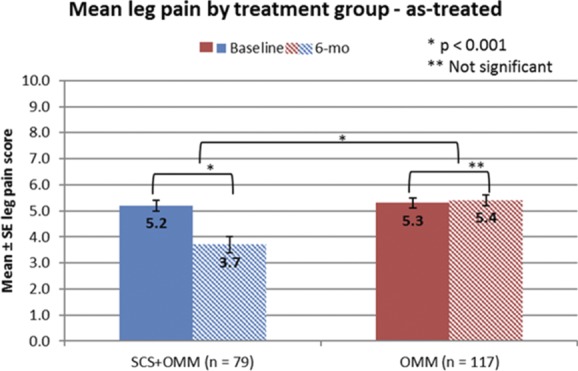
Despite optimal medical management (OMM), low back pain (LBP) can be disabling, particularly after spinal surgery. Spinal cord stimulation (SCS) is effective in reducing neuropathic leg pain; however, evidence is limited for LBP. This prospective, open-label, parallel-group trial randomized (1:1) failed back surgery syndrome (FBSS) patients with predominant LBP to SCS plus OMM (SCS group) or OMM alone (OMM group) at 28 sites in Europe and the Americas. If trial stimulation was successful, a multicolumn SCS system was implanted. Outcomes were assessed at baseline (before randomization) and at 1, 3, 6, and 12 months after randomization. Patients could change treatment groups at 6 months. The primary outcome was the proportion of patients with ≥50% reduction in LBP (responder) at 6 months. Secondary outcomes included change in pain intensity, functional disability, and health-related quality of life (HRQoL). The results are posted at ClinicalTrials.gov under registration number NCT01697358. In the intent-to-treat analysis, there were more responders in the SCS group than in the OMM group (13.6%, 15/110 vs 4.6%, 5/108, difference 9% with 95% confidence interval 0.6%-17.5%, P = 0.036) at 6 months. The SCS group improved in all secondary outcomes compared with the OMM group. The OMM group only improved in HRQoL. In the SCS group, 17.6% (18/102) experienced SCS-related adverse events through 6 months, with 11.8% (12/102) requiring surgical reintervention. Adding multicolumn SCS to OMM improved pain relief, HRQoL, and function in a traditionally difficult-to-treat population of failed back surgery syndrome patients with predominant LBP. Improvements were sustained at 12 and 24 months.
Conflict of interest statement
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures


Comment in
-
Spinal cord stimulation for failed back surgery: all that glitters is not gold.Pain. 2019 Aug;160(8):1903-1904. doi: 10.1097/j.pain.0000000000001605. Pain. 2019. PMID: 31335660 No abstract available.
-
Reply to Tapia et al.Pain. 2019 Aug;160(8):1904. doi: 10.1097/j.pain.0000000000001603. Pain. 2019. PMID: 31335661 No abstract available.
References
-
- Bouhassira D, Attal N, Alchaar H, Boureau F, Brochet B, Bruxelle J, Cunin G, Fermanian J, Ginies P, Grun-Overdyking A, Jafari-Schluep H, Lantéri-Minet M, Laurent B, Mick G, Serrie A, Valade D, Vicaut E. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). PAIN 2005;114:29–36. - PubMed
-
- Buysse DJ, Reynolds CF, III, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 1989;28:193–213. - PubMed
-
- Chan CW, Peng P. Failed back surgery syndrome. Pain Med 2011;12:577–606. - PubMed
-
- Chapman JR, Norvell DC, Hermsmeyer JT, Bransford RJ, DeVine J, McGirt MJ, Lee MJ. Evaluating common outcomes for measuring treatment success for chronic low back pain. Spine (Phila PA 1976) 2011;36(21 suppl):S54–68. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
