

Effect of Electroencephalography-Guided Anesthetic Administration on Postoperative Delirium Among Older Adults Undergoing Major Surgery: The ENGAGES Randomized Clinical Trial
- PMID: 30721296
- PMCID: PMC6439616
- DOI: 10.1001/jama.2018.22005
Effect of Electroencephalography-Guided Anesthetic Administration on Postoperative Delirium Among Older Adults Undergoing Major Surgery: The ENGAGES Randomized Clinical Trial
Abstract
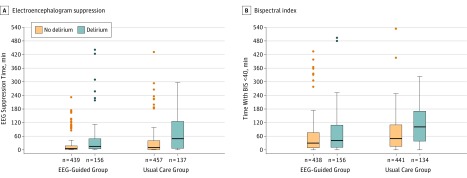
Importance: Intraoperative electroencephalogram (EEG) waveform suppression, often suggesting excessive general anesthesia, has been associated with postoperative delirium.
Objective: To assess whether EEG-guided anesthetic administration decreases the incidence of postoperative delirium.
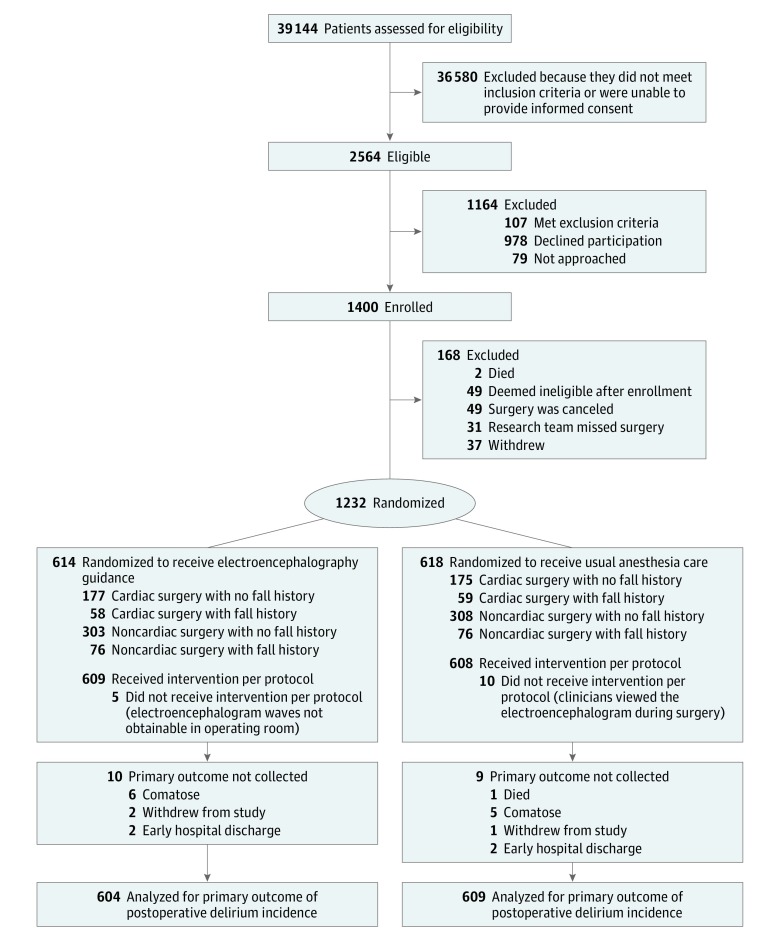
Design, setting, and participants: Randomized clinical trial of 1232 adults aged 60 years and older undergoing major surgery and receiving general anesthesia at Barnes-Jewish Hospital in St Louis. Recruitment was from January 2015 to May 2018, with follow-up until July 2018.
Interventions: Patients were randomized 1:1 (stratified by cardiac vs noncardiac surgery and positive vs negative recent fall history) to receive EEG-guided anesthetic administration (n = 614) or usual anesthetic care (n = 618).
Main outcomes and measures: The primary outcome was incident delirium during postoperative days 1 through 5. Intraoperative measures included anesthetic concentration, EEG suppression, and hypotension. Adverse events included undesirable intraoperative movement, intraoperative awareness with recall, postoperative nausea and vomiting, medical complications, and death.
Results: Of the 1232 randomized patients (median age, 69 years [range, 60 to 95]; 563 women [45.7%]), 1213 (98.5%) were assessed for the primary outcome. Delirium during postoperative days 1 to 5 occurred in 157 of 604 patients (26.0%) in the guided group and 140 of 609 patients (23.0%) in the usual care group (difference, 3.0% [95% CI, -2.0% to 8.0%]; P = .22). Median end-tidal volatile anesthetic concentration was significantly lower in the guided group than the usual care group (0.69 vs 0.80 minimum alveolar concentration; difference, -0.11 [95% CI, -0.13 to -0.10), and median cumulative time with EEG suppression was significantly less (7 vs 13 minutes; difference, -6.0 [95% CI, -9.9 to -2.1]). There was no significant difference between groups in the median cumulative time with mean arterial pressure below 60 mm Hg (7 vs 7 minutes; difference, 0.0 [95% CI, -1.7 to 1.7]). Undesirable movement occurred in 137 patients (22.3%) in the guided and 95 (15.4%) in the usual care group. No patients reported intraoperative awareness. Postoperative nausea and vomiting was reported in 48 patients (7.8%) in the guided and 55 patients (8.9%) in the usual care group. Serious adverse events were reported in 124 patients (20.2%) in the guided and 130 (21.0%) in the usual care group. Within 30 days of surgery, 4 patients (0.65%) in the guided group and 19 (3.07%) in the usual care group died.
Conclusions and relevance: Among older adults undergoing major surgery, EEG-guided anesthetic administration, compared with usual care, did not decrease the incidence of postoperative delirium. This finding does not support the use of EEG-guided anesthetic administration for this indication.
Trial registration: ClinicalTrials.gov Identifier: NCT02241655.
Conflict of interest statement
Figures
Comment in
-
Depth of Anesthesia and Postoperative Delirium.JAMA. 2019 Feb 5;321(5):459-460. doi: 10.1001/jama.2019.0164. JAMA. 2019. PMID: 30721279 No abstract available.
-
Electroencephalography-guided anaesthetic administration does not impact postoperative delirium among older adults undergoing major surgery: an independent discussion of the ENGAGES trial.Br J Anaesth. 2019 Aug;123(2):112-117. doi: 10.1016/j.bja.2019.03.016. Epub 2019 May 10. Br J Anaesth. 2019. PMID: 31079835 Free PMC article. No abstract available.
-
Electroencephalography-Guided Anesthetic Administration and Postoperative Delirium.JAMA. 2019 Jun 25;321(24):2469-2470. doi: 10.1001/jama.2019.5145. JAMA. 2019. PMID: 31237632 No abstract available.
-
Electroencephalography-Guided Anesthetic Administration and Postoperative Delirium.JAMA. 2019 Jun 25;321(24):2470-2471. doi: 10.1001/jama.2019.5149. JAMA. 2019. PMID: 31237633 No abstract available.
-
Electroencephalography-Guided Anesthetic Administration and Postoperative Delirium.JAMA. 2019 Jun 25;321(24):2470. doi: 10.1001/jama.2019.5157. JAMA. 2019. PMID: 31237634 No abstract available.
-
[Influence of EEG-guided administration of anesthesia on postoperative delirium in older patients].Anaesthesist. 2019 Jul;68(7):483-484. doi: 10.1007/s00101-019-0624-9. Anaesthesist. 2019. PMID: 31286162 German. No abstract available.
-
A call for a more rigorous screening of postoperative delirium.Ann Transl Med. 2019 Sep;7(Suppl 6):S192. doi: 10.21037/atm.2019.07.32. Ann Transl Med. 2019. PMID: 31656771 Free PMC article. No abstract available.
References
-
- Avidan MS, Maybrier HR, Abdallah AB, et al. Intraoperative ketamine for prevention of postoperative delirium or pain after major surgery in older adults: an international, multicentre, double-blind, randomised clinical trial. Lancet. 2017;390(10091):267-275. doi: 10.1016/S0140-6736(17)31467-8 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
