

The cost-effectiveness of osteochondral allograft transplantation in the knee
- PMID: 30721344
- PMCID: PMC6541582
- DOI: 10.1007/s00167-019-05392-8
The cost-effectiveness of osteochondral allograft transplantation in the knee
Abstract
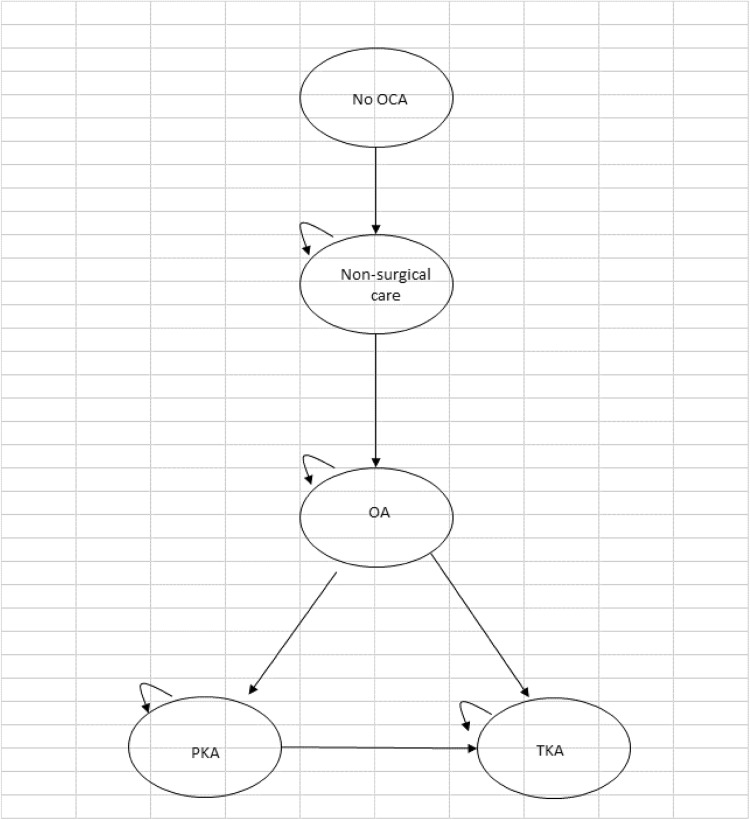
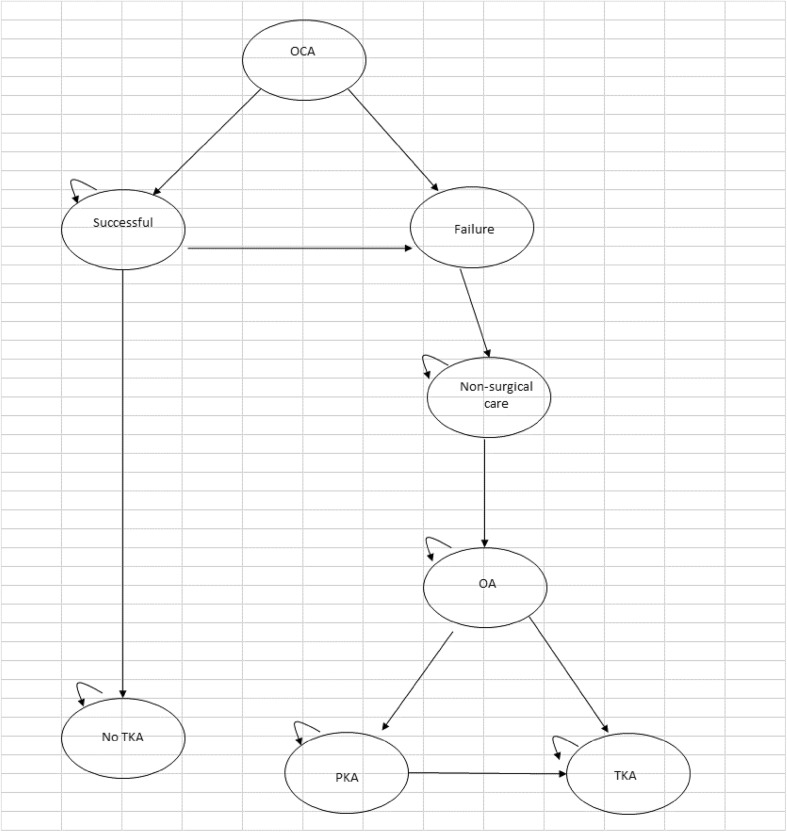
Purpose: Osteochondral allografts (OCA) consist of a layer of hyaline cartilage and a layer of underlying bone. They are used to repair combined defects of articular cartilage and bone. Such defects often occur in people far too young to have knee arthroplasty, for whom the main alternative to OCA is conservative symptomatic care, which will not prevent development of osteoarthritis. The aim of this report was to assess the cost-effectiveness of osteochondral allograft transplantation in the knee.
Methods: Systematic review of evidence on clinical effectiveness and economic modelling.
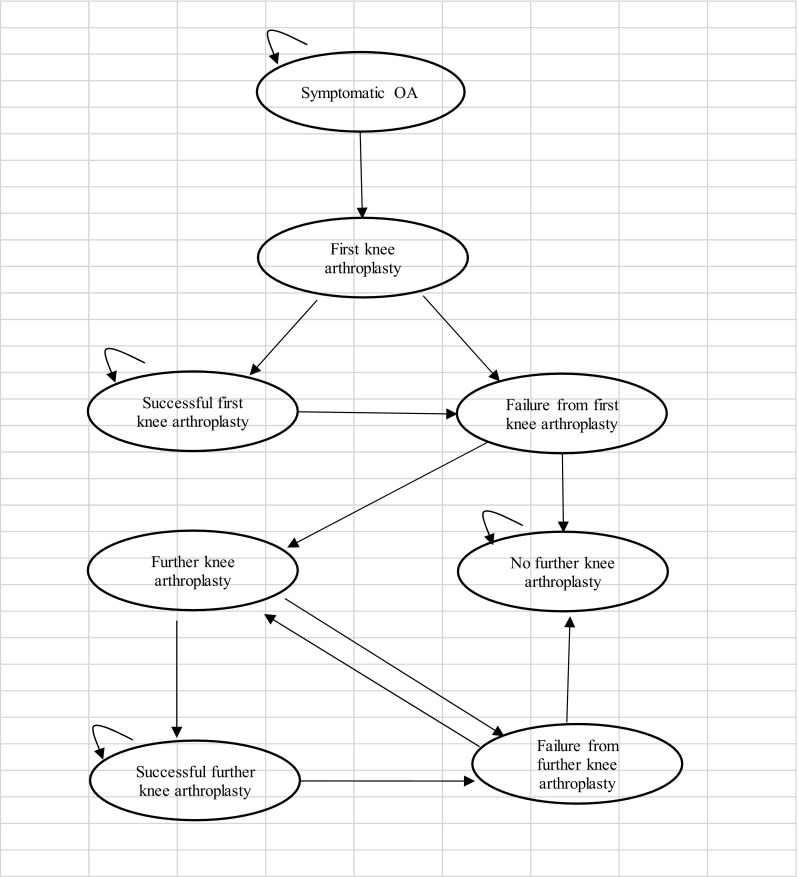
Results: The evidence on osteochondral allograft transplantation comes from observational studies, but often based on good quality prospective registries of all patients having such surgery. Without controlled trials, it was necessary to use historical cohorts to assess the effect of osteochondral grafts. There is good evidence that OCA are clinically effective with a high graft survival rate over 20 years. If an OCA graft fails, there is some evidence that revision with a second OCA is also effective, though less so than primary OCA. Economic modelling showed that osteochondral allograft transplantation was highly cost-effective, with costs per quality adjusted life year much lower than many other treatments considered cost effective.
Conclusions: Osteochondral allograft transplantation appears highly cost-effective though the cost per quality adjusted life year varies according to the widely varying costs of allografts. Based on one small study, revision OCA also appears very cost-effective, but more evidence is needed.
Level of evidence: II.
Keywords: Allografts; Cost-effectiveness; Osteochondral; Systematic review.
Conflict of interest statement
The authors declare that they have no potential conflict of interest.
Figures
References
-
- Bayliss LE, Culliford D, Monk AP, Glyn-Jones S, Prieto-Alhambra D, Judge A, et al. The effect of patient age at intervention on risk of implant revision after total replacement of the hip or knee: a population-based cohort study. Lancet. 2017;389:1424–1430. doi: 10.1016/S0140-6736(17)30059-4. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
