

Elaboration of Consensus Clinical Endpoints to Evaluate Antimicrobial Treatment Efficacy in Future Hospital-acquired/Ventilator-associated Bacterial Pneumonia Clinical Trials
- PMID: 30722013
- PMCID: PMC9431655
- DOI: 10.1093/cid/ciz093
Elaboration of Consensus Clinical Endpoints to Evaluate Antimicrobial Treatment Efficacy in Future Hospital-acquired/Ventilator-associated Bacterial Pneumonia Clinical Trials
Abstract
Background: Randomized clinical trials (RCTs) in hospital-acquired and ventilator-associated bacterial pneumonia (HABP and VABP, respectively) are important for the evaluation of new antimicrobials. However, the heterogeneity in endpoints used in RCTs evaluating treatment of HABP/VABP may puzzle clinicians. The aim of this work was to reach a consensus on clinical endpoints to consider in future clinical trials evaluating antimicrobial treatment efficacy for HABP/VABP.
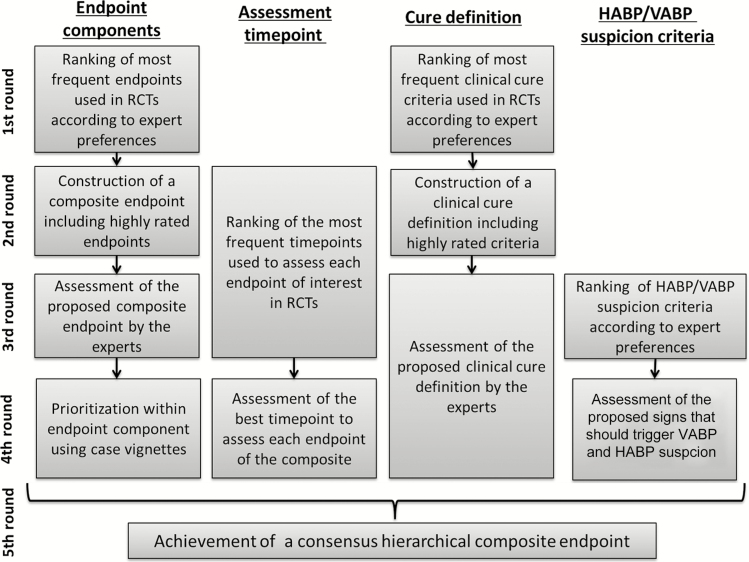
Methods: Twenty-six international experts from intensive care, infectious diseases, and the pharmaceutical industry were polled using the Delphi method.
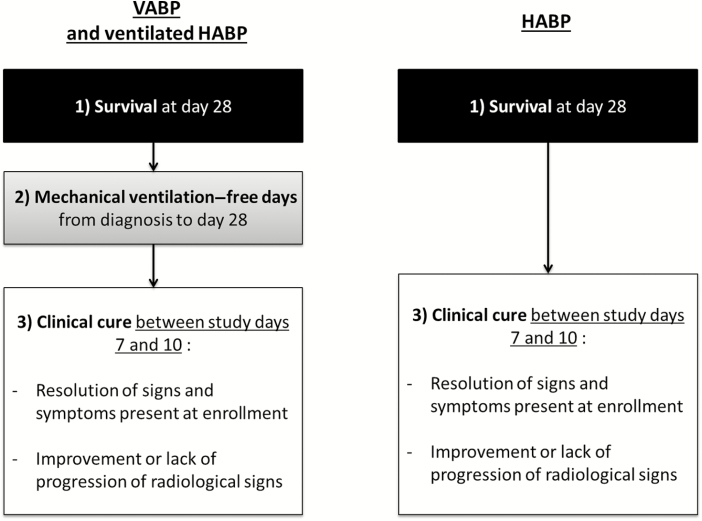
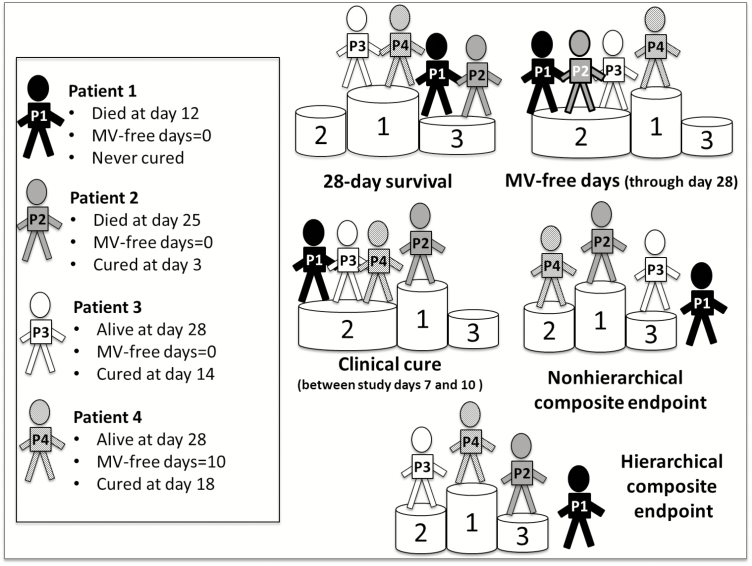
Results: The panel recommended a hierarchical composite endpoint including, by priority order, (1) survival at day 28, (2) mechanical ventilation-free days through day 28, and (3) clinical cure between study days 7 and 10 for VABP; and (1) survival (day 28) and (2) clinical cure (days 7-10) for HABP. Clinical cure was defined as the combination of resolution of signs and symptoms present at enrollment and improvement or lack of progression of radiological signs. More than 70% of the experts agreed to assess survival and mechanical ventilation-free days though day 28, and clinical cure between day 7 and day 10 after treatment initiation. Finally, the hierarchical order of endpoint components was reached after 3 Delphi rounds (72% agreement).
Conclusions: We provide a multinational expert consensus on separate hierarchical composite endpoints for VABP and HABP, and on a definition of clinical cure that could be considered for use in future HABP/VABP clinical trials.
Keywords: Delphi method; clinical cure; hierarchical composite endpoint; hospital-acquired bacterial pneumonia; multinational consensus.
© The Author(s) 2019. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Torres A, Niederman MS, Chastre J, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociacion Latinoamericana del Torax (ALAT). Eur Respir J 2017; 50. doi: 10.1183/13993003.00582-2017. - DOI - PubMed
-
- US Food and Drug Administration Center for Drug Evaluation and Research . Guidance for industry hospital-acquired bacterial pneumonia and ventilator- associated bacterial pneumonia: developing drugs for treatment. XXX: US Department of Health and Human Services, 2014.
-
- European Medicines Agency. Addendum to the guideline on the evaluation of medicinal products indicated for treatment of bacterial infections. London, UK: EMA, 2013.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
