

Review
doi: 10.1161/CIRCEP.118.006816.
Device Programming for His Bundle Pacing
Affiliations
- PMID: 30722682
- PMCID: PMC6420120
- DOI: 10.1161/CIRCEP.118.006816
Item in Clipboard
Review
Device Programming for His Bundle Pacing
Circ Arrhythm Electrophysiol.
2019 Feb.
Abstract
Although permanent His bundle pacing was first reported almost 2 decades ago, it is only recently gaining wider adoption, following facilitation of the implant procedure by dedicated tools. An additional challenge is programming the system, as His bundle pacing may have specific configurations and require special considerations which current implantable pulse generators are not designed for. The aim of this article is to provide practical recommendations for programming His bundle pacing, to deliver optimal therapy and ensure patient safety.
Keywords: bundle of His; cardiac pacemaker, artificial; cardiac resynchronization therapy; defibrillators; patient safety.
Figures
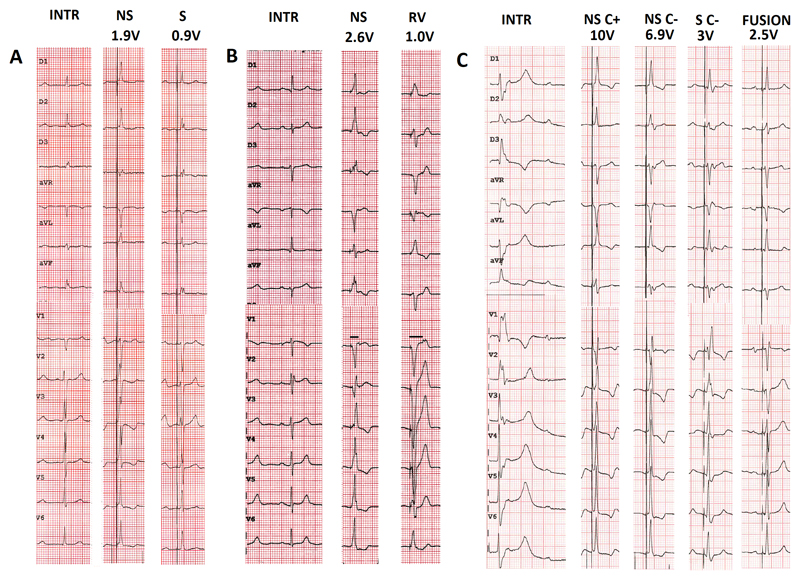
Examples of types of His capture at different programmed pacing outputs in three patients. A. Patient in atrial fibrillation awaiting atrioventricular nodal ablation. Transition from non-selective to selective His capture. Note the presence of a pseudo-delta wave without an isoelectric interval after the pacing spike with non-selective capture, visible in aVL and the precordial leads B. Patient with exercise-induced Mobitz 2 atrioventricular block and narrow intrinsic QRS. Transition from non-selective His capture to right ventricular capture. Note the increase in stimulus to retrograde P duration with right ventricular capture compared to during His bundle capture (horizontal lines in lead V1). C. Patient in sinus rhythm with complete atrioventricular block and ventricular escape rhythm. Selective capture without correction shows a typical right bundle branch block pattern. Note how it is difficult to distinguish between non-selective capture with and without correction (a difference in QRS morphology is visible in lead II). The patient had a biventricular pacemaker with an atrial, right ventricular, and His lead (connected to the left ventricular port). Due to high capture thresholds for non-selective His capture, fusion pacing with sequential selective His capture (threshold was 1.5V/0.5ms) and right ventricular pacing was programmed. INTR: intrinsic rhythm; NS: non-selective His capture; S: selective His capture; C+: with correction; C-: without correction.
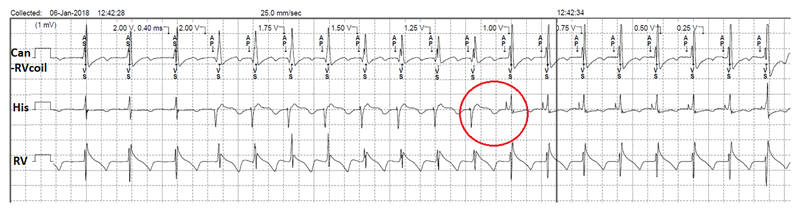
Threshold test with 0.4ms pulse width with the His lead connected to the atrial port of a dual-chamber pacemaker. Non-selective His capture down to 1V, with selective capture thereafter (down to the minimum amplitude of 0.25V). Note the change in electrogram morphology during the transition of non-selective to selective capture (circle). This patient had underlying right bundle branch block, which explains why sensed events by the His lead are labelled as “AS” and not “Ab”.
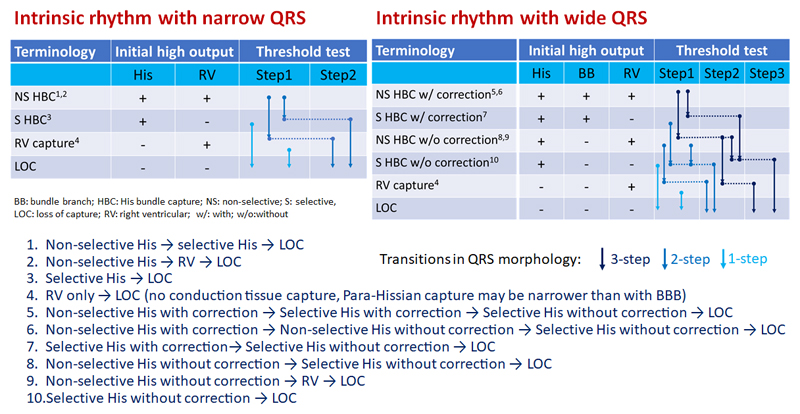
Summary of the main possible transitions during threshold testing of direct His bundle pacing. Note that only initial selective His bundle capture or initial right ventricular myocardial capture (without His capture) result in a single step. Transitions may however be missed if the decrement in pacing output is greater than the difference in thresholds (e.g. between myocardial and His thresholds). Additional minor transitions are possible in case of varying degrees of correction of BBB in a given patient, or with anodal capture if the His lead is programmed to a bipolar or extended bipolar vector, and are not shown here.
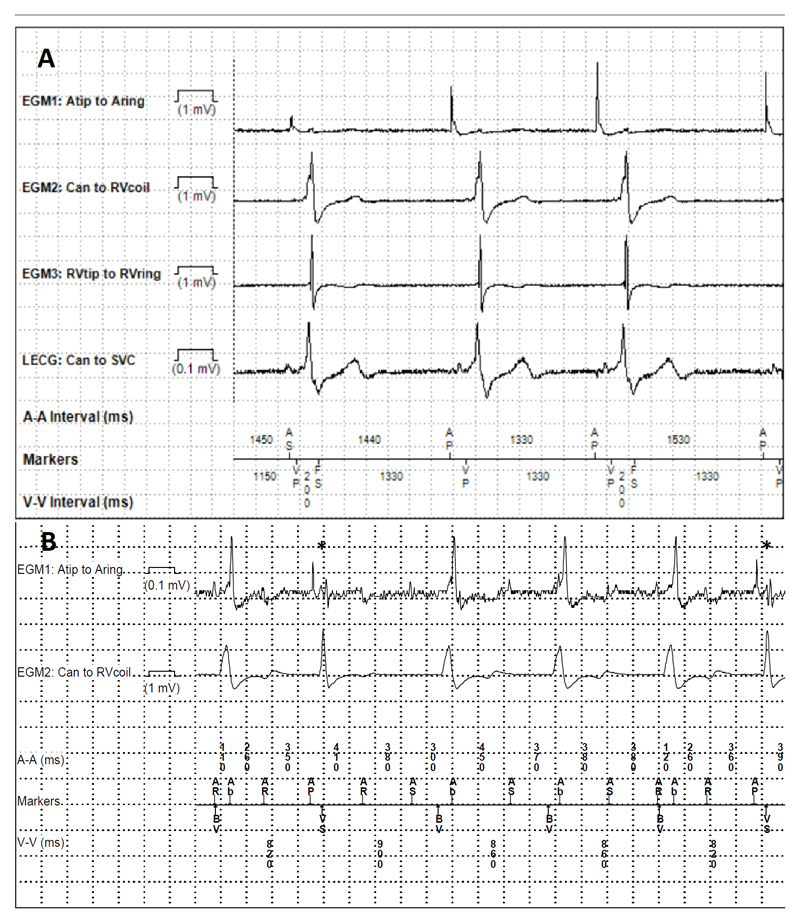
Oversensing issues with HBP. A. Ventricular double-counting. Biventricular defibrillator with a His lead connected to the left ventricular port. Pacing from the His lead only, with sensing from the right ventricular channel at 200ms as shown by the “FS” (fibrillation sense) events (first and third cycles). Ventricular blanking was extended from 200ms to 230ms, which solved the issue. B. Atrial oversensing. Patient in atypical flutter who had undergone atrioventricular nodal ablation, implanted with a biventricular defibrillator and a His lead connected to the atrial port with nominal sensitivity settings. Note sensing of the atrial flutter in the His lead, with mode switch and pacing in the DDIR mode at the baseline rate of 70bpm, mostly with biventricular pacing, and inhibition of His bundle pacing except in two instances denoted by the asterisks. Atrial sensitivity was decreased from 0.3mV to 4mV, with resumption of His pacing.
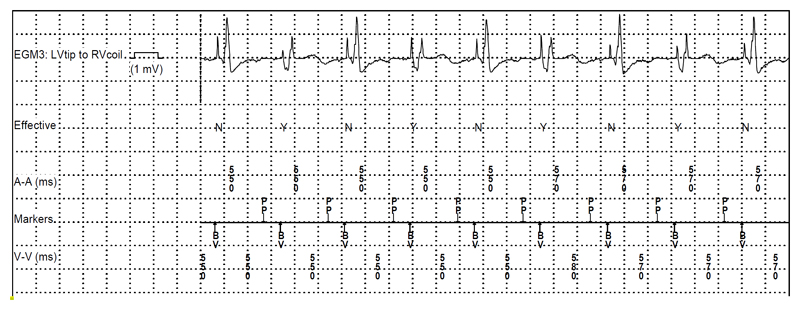
Episode of an “ineffective” ventricular capture event retrieved from a patient with a His lead connected to the left ventricular port of a biventricular defibrillator (with His pacing in lieu of biventricular pacing due to anomaly of the coronary sinus). The Medtronic EffectivCRT algorithm annotates “ineffective” capture cycles with an “N”, which correspond in this case to selective His capture and “effective” cycles with a “Y”, which correspond here to non-selective capture (markers are displayed in the second line). Note the differences in electrogram morphology with “QR” waveforms of the “effective” cycles corresponding to local myocardial capture of non-selective His capture and an isoelectric interval with a far-field ventricular electrogram corresponding to the “ineffective” cycle (selective His capture). It could be deduced from the counters that the patient had selective His capture in 98% of the time (the threshold for selective capture was 1.0V/0.4ms and for non-selective capture, 2.75V/0.4ms, with a programmed output of 2.5V/0.4ms). This patient also had episodes of ectopic atrial rhythm originating close to the coronary sinus with short PR intervals, resulting in loss of His pacing; the “preferential pacing” algorithm was activated to override this rhythm (indicated by the “PP” annotation of the atrial marker channel).
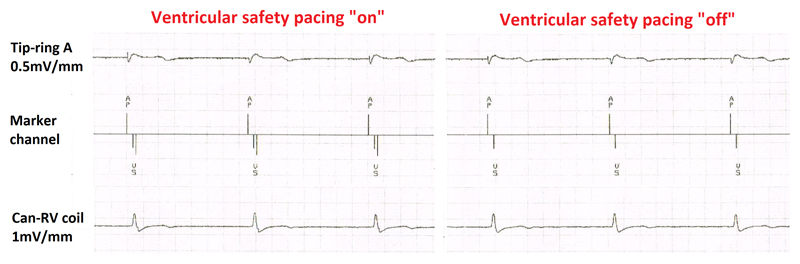
Medtronic biventricular defibrillator in a patient in atrial fibrillation who had undergone atrioventricular nodal ablation. Left: Pacing by the His lead connected to the atrial port with detection of the local ventricular electrogram by the right ventricular lead after approximately 80ms, which triggers ventricular safety pacing (depicted in Medtronic devices by the double downward lines in the marker channel) at the end of the 110ms window. Right: After inactivation of ventricular safety pacing (after having ruled out crosstalk), unnecessary ventricular pacing with pseudofusion is avoided.
References
-
- Deshmukh P, Casavant DA, Romanyshyn M, Anderson K. Permanent, direct His-bundle pacing: a novel approach to cardiac pacing in patients with normal His-Purkinje activation. Circulation. 2000;101:869–77. - PubMed
-
- Barba-Pichardo R, Moriña-Vázquez P, Venegas-Gamero J, Maroto-Monserrat F, Cid-Cumplido M, Herrera-Carranza M. Permanent His-Bundle Pacing in Patients With Infra-Hisian Atrioventricular Block. Revista Española de Cardiología (English Edition) 2006;59:553–558. - PubMed
-
- Sharma PS, Dandamudi G, Naperkowski A, Oren JW, Storm RH, Ellenbogen KA, Vijayaraman P. Permanent His-bundle pacing is feasible, safe, and superior to right ventricular pacing in routine clinical practice. Heart Rhythm. 2015;12:305–12. - PubMed
-
- Zanon F, Ellenbogen KA, Dandamudi G, Sharma PS, Huang W, Lustgarten DL, Tung R, Tada H, Koneru JN, Bergemann T, Fagan DH, et al. Permanent His-bundle pacing: a systematic literature review and meta-analysis. EP Europace. 2018 in press. - PubMed
-
- Vijayaraman P, Chung MK, Dandamudi G, Upadhyay GA, Krishnan K, Crossley G, Bova Campbell K, Lee BK, Refaat MM, Saksena S, Fisher JD, et al. His Bundle Pacing. Journal of the American College of Cardiology. 2018;72:927–947. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
