

Association of Fetal Growth With General and Specific Mental Health Conditions
- PMID: 30725083
- PMCID: PMC6495458
- DOI: 10.1001/jamapsychiatry.2018.4342
Association of Fetal Growth With General and Specific Mental Health Conditions
Abstract
Importance: It is unclear if the associations between fetal growth and later mental health conditions remain after controlling for familial factors and psychiatric comorbidity.
Objective: To examine the associations between fetal growth and general and specific mental health conditions, controlling for familial factors.
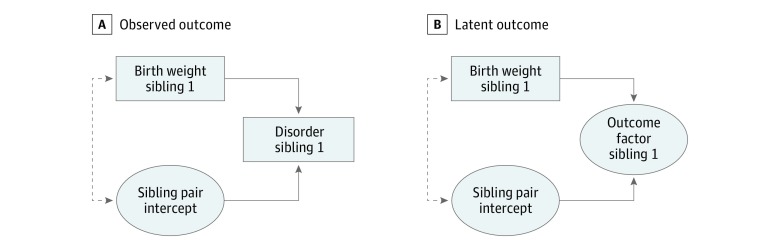
Design, setting, and participants: This register-based study conducted in Sweden analyzed 546 894 pairs of full siblings born between January 1, 1973, and December 31, 1998. Sibling pairs were followed up through December 31, 2013. First, population-based and within-sibling pair associations (which controlled for time-invariant familial confounders) between fetal growth and the outcomes were estimated. Second, exploratory factor analysis was applied to the outcomes to derive 1 general factor and 4 specific and independent factors. Third, the general and specific factors were regressed on fetal growth. Statistical analysis was performed from March 27, 2017, to October 27, 2018.
Main outcome and measures: The outcomes were 11 psychiatric diagnoses (depression, anxiety, obsessive-compulsive disorder, posttraumatic stress disorder, bipolar disorder, alcohol abuse, drug use, attention-deficit/hyperactivity disorder, autism, schizophrenia, and schizoaffective disorder) and court convictions of violent crimes. Birth weight (in kilograms) statistically adjusted for gestational age was the exposure.
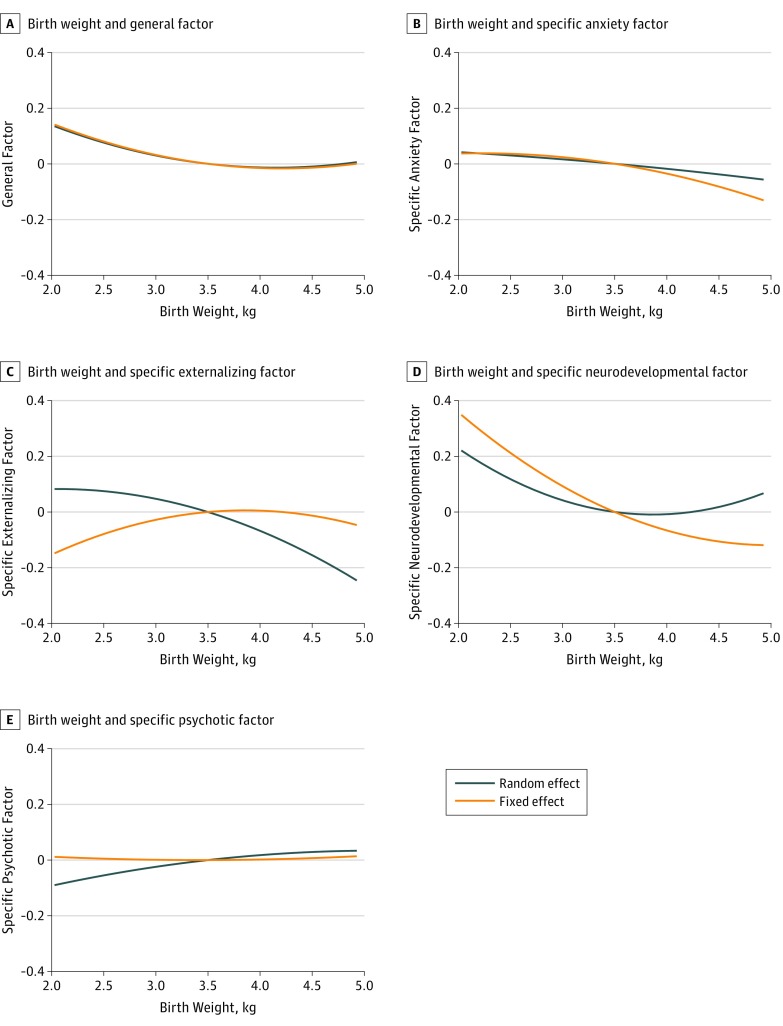
Results: The mean (SD) age of the 1 093 788 participants was 27.2 (6.8) years (range, 15.1-40.9 years) and 51.5% were male. Nine outcomes were significantly associated with birth weight in the population at large: depression (odds ratio [OR], 0.96; 95% CI, 0.95-0.98), anxiety (OR, 0.94; 95% CI, 0.92-0.95), posttraumatic stress disorder (OR, 0.91; 95% CI, 0.89-0.93), bipolar disorder (OR, 0.94; 95% CI, 0.89-1.00), alcohol abuse (OR, 0.89; 95% CI, 0.87-0.91), drug use (OR, 0.83; 95% CI, 0.80-0.85), violent crimes (OR, 0.85; 95% CI, 0.83-0.86), attention-deficit/hyperactivity disorder (OR, 0.88; 95% CI, 0.86-0.90), and autism (OR, 0.95; 95% CI, 0.92-0.97). Only depression (OR, 0.95; 95% CI 0.92-0.98), obsessive-compulsive disorder (OR, 0.93; 95% CI, 0.87-0.99), attention-deficit/hyperactivity disorder (OR, 0.86; 95% CI, 0.82-0.89), and autism (OR, 0.72; 95% CI, 0.69-0.76) remained significantly associated within sibling pairs. An exploratory factor analysis indicated that 1 general and 4 specific factors (capturing anxiety, externalizing, neurodevelopmental, and psychotic conditions) fit the outcomes well. Across almost all sensitivity analyses, an increase in birth weight by 1 kg significantly reduced the general (β, -0.047; 95% CI, -0.071 to -0.023) and the specific neurodevelopmental factors (β, -0.159; 95% CI, -0.190 to -0.128) within sibling pairs.
Conclusions and relevance: Controlling for familial confounders, reduced fetal growth was associated with a small but significant increase in the general factor of psychopathology and a moderate increase in a specific neurodevelopmental factor.
Conflict of interest statement
Figures
Comment in
-
Exploring the Association of Sex Differences and Exposure to Maternal Smoking With Low Fetal Growth-Reply.JAMA Psychiatry. 2019 Jul 1;76(7):767-768. doi: 10.1001/jamapsychiatry.2019.1127. JAMA Psychiatry. 2019. PMID: 31141095 No abstract available.
-
Exploring the Association of Sex Differences and Exposure to Maternal Smoking With Low Fetal Growth.JAMA Psychiatry. 2019 Jul 1;76(7):766-767. doi: 10.1001/jamapsychiatry.2019.1116. JAMA Psychiatry. 2019. PMID: 31141096 No abstract available.
-
Exploring the Association of Sex Differences and Exposure to Maternal Smoking With Low Fetal Growth.JAMA Psychiatry. 2019 Jul 1;76(7):766. doi: 10.1001/jamapsychiatry.2019.1130. JAMA Psychiatry. 2019. PMID: 31141101 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
