

Development and Validation of a Prediction Model for Prehospital Triage of Trauma Patients
- PMID: 30725101
- PMCID: PMC6537785
- DOI: 10.1001/jamasurg.2018.4752
Development and Validation of a Prediction Model for Prehospital Triage of Trauma Patients
Abstract
Importance: Prehospital trauma triage protocols are used worldwide to get the right patient to the right hospital and thereby improve the chance of survival and avert lifelong disabilities. The American College of Surgeons Committee on Trauma set target levels for undertriage rates of less than 5%. None of the existing triage protocols has been able to achieve this target in isolation.
Objective: To develop and validate a new prehospital trauma triage protocol to improve current triage rates.
Design, setting, and participants: In this multicenter cohort study, all patients with trauma who were 16 years and older and transported to a trauma center in 2 different regions of the Netherlands were included in the analysis. Data were collected from January 1, 2012, through June 30, 2014, in the Central Netherlands region for the design data cohort and from January 1 through December 31, 2015, in the Brabant region for the validation cohort. Data were analyzed from May 3, 2017, through July 19, 2018.
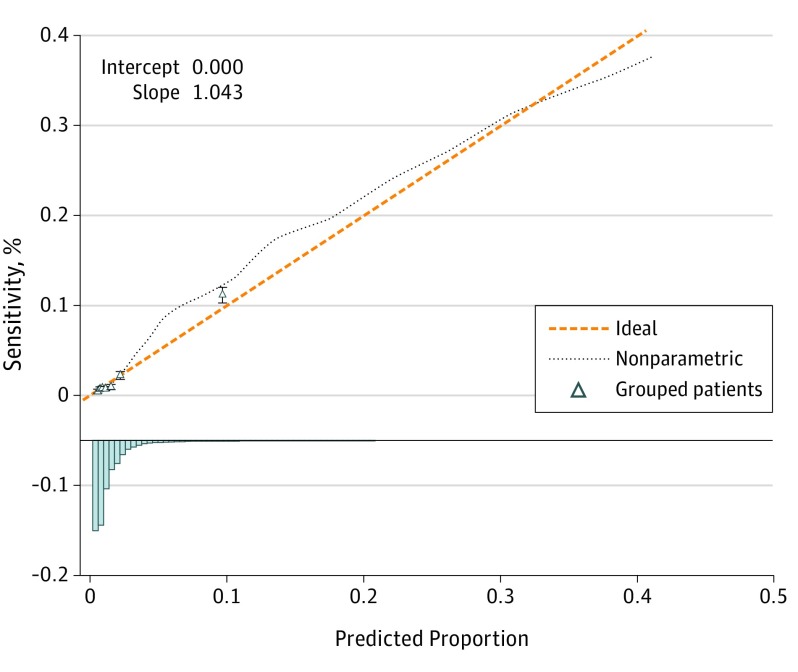
Main outcomes and measures: A new prediction model was developed in the Central Netherlands region based on prehospital predictors associated with severe injury. Severe injury was defined as an Injury Severity Score greater than 15. A full-model strategy with penalized maximum likelihood estimation was used to construct a model with 8 predictors that were chosen based on clinical reasoning. Accuracy of the developed prediction model was assessed in terms of discrimination and calibration. The model was externally validated in the Brabant region.
Results: Using data from 4950 patients with trauma from the Central Netherlands region for the design data set (58.3% male; mean [SD] age, 47 [21] years) and 6859 patients for the validation Brabant region (52.2% male; mean [SD] age, 51 [22] years), the following 8 significant predictors were selected for the prediction model: age; systolic blood pressure; Glasgow Coma Scale score; mechanism criteria; penetrating injury to the head, thorax, or abdomen; signs and/or symptoms of head or neck injury; expected injury in the Abbreviated Injury Scale thorax region; and expected injury in 2 or more Abbreviated Injury Scale regions. The prediction model showed a C statistic of 0.823 (95% CI, 0.813-0.832) and good calibration. The cutoff point with a minimum specificity of 50.0% (95% CI, 49.3%-50.7%) led to a sensitivity of 88.8% (95% CI, 87.5%-90.0%). External validation showed a C statistic of 0.831 (95% CI, 0.814-0.848) and adequate calibration.
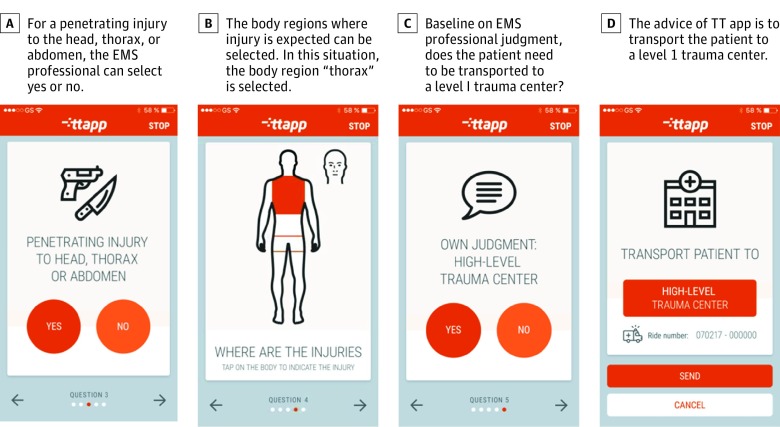
Conclusions and relevance: The new prehospital trauma triage prediction model may lower undertriage rates to approximately 10% with an overtriage rate of 50%. The next step should be to implement this prediction model with the use of a mobile app for emergency medical services professionals.
Conflict of interest statement
Figures
Comment in
-
Optimizing Prehospital Trauma Triage-A Step Closer?JAMA Surg. 2019 May 1;154(5):429-430. doi: 10.1001/jamasurg.2018.4764. JAMA Surg. 2019. PMID: 30725075 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
