

Thyroglossal duct pathology and mimics
- PMID: 30725193
- PMCID: PMC6365310
- DOI: 10.1186/s13244-019-0694-x
Thyroglossal duct pathology and mimics
Abstract
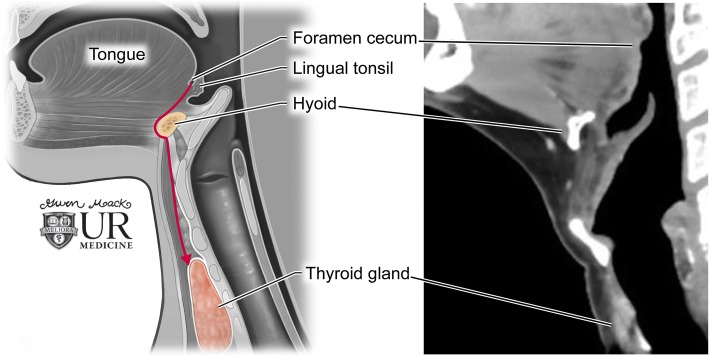
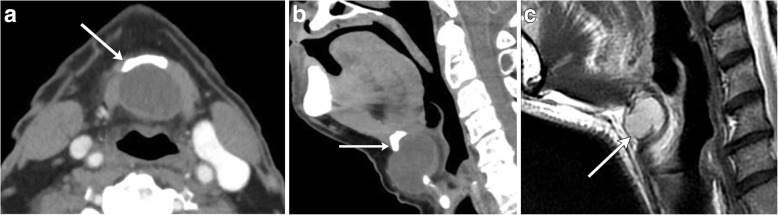
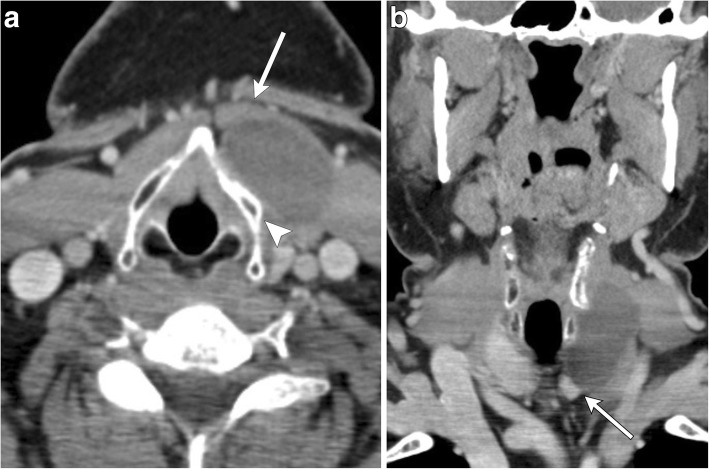
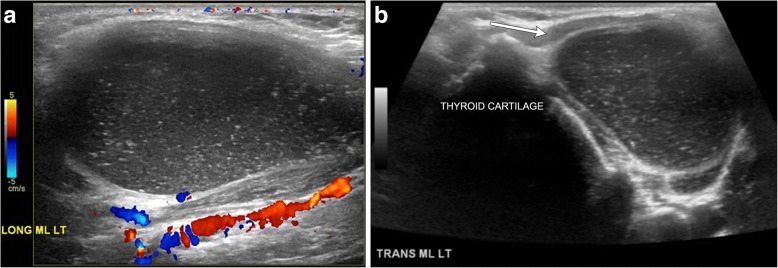
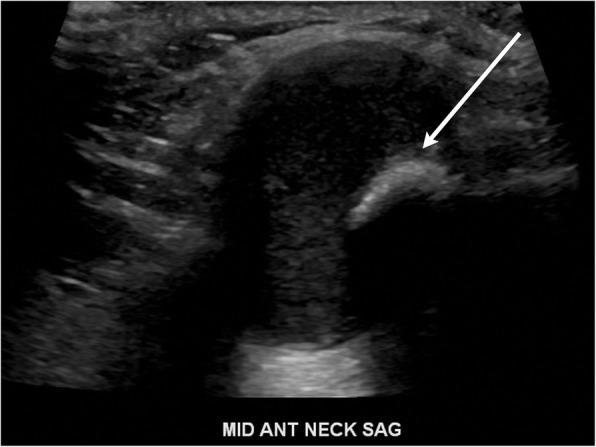
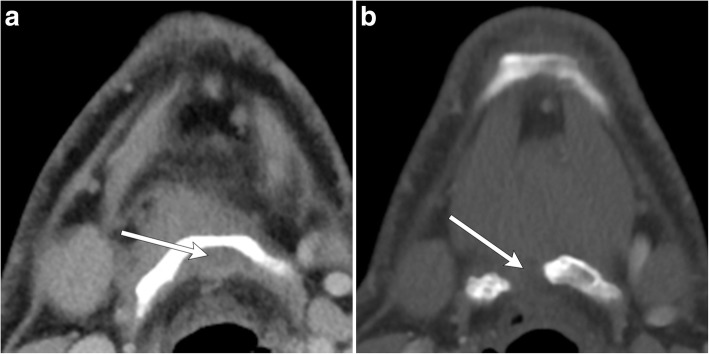
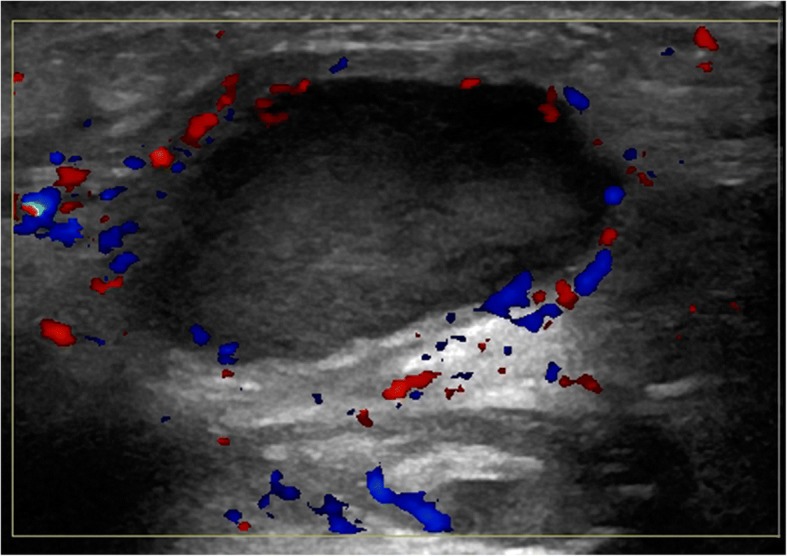
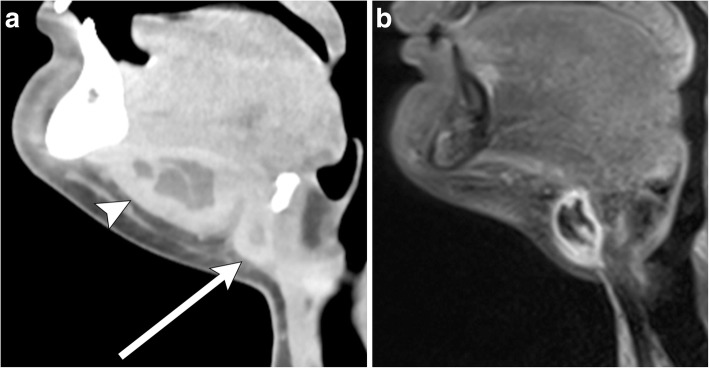
Congenital anterior neck masses comprise a rare group of lesions typically diagnosed in childhood. Most commonly, lesions are anomalies of the thyroglossal duct, namely the thyroglossal duct cyst, along with ectopic thyroid tissue. Although usually suspected based on clinical examination, imaging can confirm the diagnosis, assess the extent, and evaluate for associated complications. Imaging characteristics on ultrasound, CT, and MRI may at times be equivocal; differential considerations include branchial cleft cyst, dermoid/epidermoid, laryngocele, thymic cyst, lymphatic malformation, and metastatic disease. Thus, understanding of the embryologic course of thyroid development is crucial with recognition of critical landmarks such as the foramen cecum, hyoid bone, thyroid cartilage, and strap musculature to aid in the diagnosis of an anterior neck mass.
Keywords: Cystic lesions; Ectopic thyroid; Neck mass; Thyroglossal duct.
Conflict of interest statement
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Imhof H, Czerny C, Hörmann M, Krestan C (2004) Tumors and tumor-like lesions of the neck: from childhood to adult. Eur Radiol 14(Suppl 4):L155–L165. 10.1007/s00330-003-2035-0 - PubMed
-
- Koeller KK, Alamo L, Adair CF, Smirniotopoulos JG (1999) Congenital cystic masses of the neck: radiologic-pathologic correlation. Radiographics 19:121–146 - PubMed
-
- Nakayama S, Kimachi K, Nakayama K, Ikebe T, Ozeki S (2009) Thyroglossal duct cyst occurring in the floor of the mouth: report of 2 cases. J Oral Maxillofac Surg 67:2690–2693 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
