

DEFUSE 3 Non-DAWN Patients
- PMID: 30727856
- PMCID: PMC6768068
- DOI: 10.1161/STROKEAHA.118.023310
DEFUSE 3 Non-DAWN Patients
Abstract
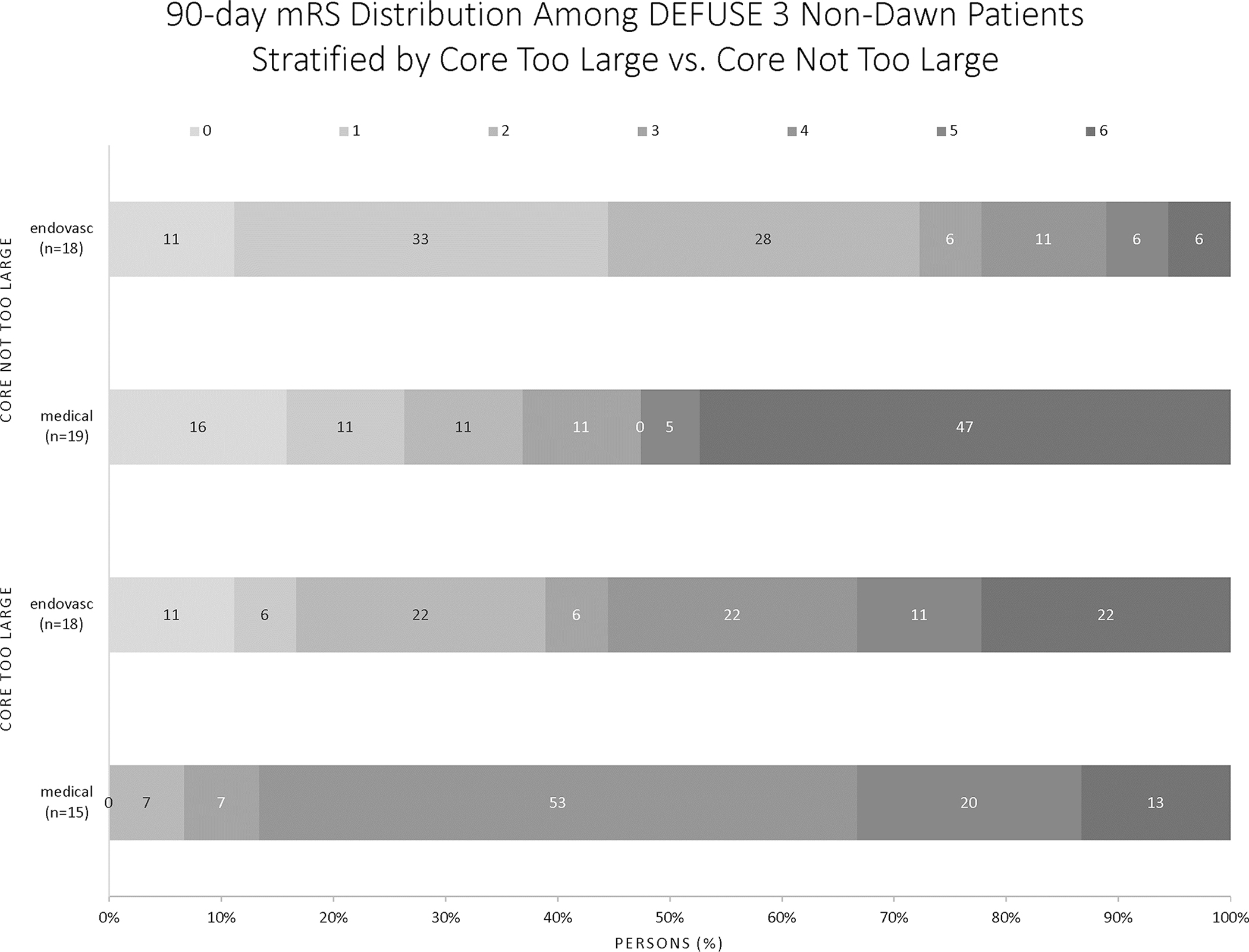
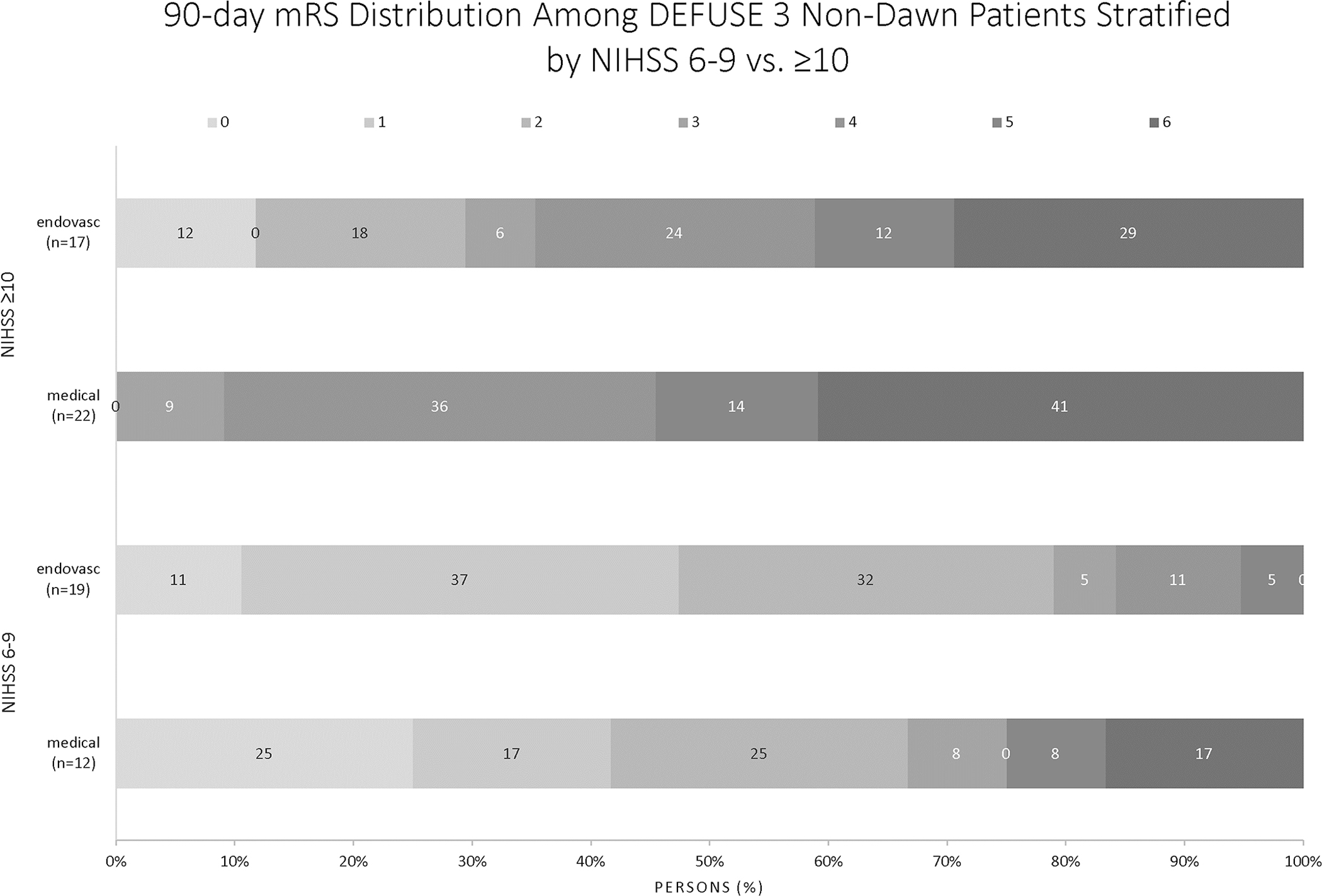
Background and Purpose- DAWN (Clinical Mismatch in the Triage of Wake Up and Late Presenting Strokes Undergoing Neurointervention With Trevo) and DEFUSE 3 (Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke) established thrombectomy for patients with emergent large vessel occlusions presenting 6 to 24 hours after symptom onset. Given the greater inclusivity of DEFUSE 3, we evaluated the effect of thrombectomy in DEFUSE 3 patients who would have been excluded from DAWN. Methods- Eligibility criteria of the DAWN trial were applied to DEFUSE 3 patient data to identify DEFUSE 3 patients not meeting DAWN criteria (DEFUSE 3 non-DAWN). Reasons for DAWN exclusion in DEFUSE 3 were infarct core too large, National Institutes of Health Stroke Scale (NIHSS) score 6 to 9, and modified Rankin Scale score of 2. Subgroups were compared with the DEFUSE 3 non-DAWN and entire DEFUSE 3 cohorts. Results- There were 71 DEFUSE 3 non-DAWN patients; 31 patients with NIHSS 6 to 9, 33 with core too large, and 13 with premorbid modified Rankin Scale score of 2 (some patients met multiple criteria). For core-too-large patients, median 24-hour infarct volume was 119 mL (interquartile range, 74.6-180) versus 31.5 mL (interquartile range, 17.6-64.3) for core-not-too-large patients ( P<0.001). Complications and functional outcomes were similar between the groups. Thrombectomy in core-too-large patients compared with the remaining DEFUSE 3 non-DAWN patients conveyed benefit for functional outcome (odds ratio, 20.9; CI, 1.3-337.8). Comparing the NIHSS 6 to 9 group with the NIHSS ≥10 patients, modified Rankin Scale score 0 to 2 outcomes were achieved in 74% versus 22% ( P<0.001), with mortality in 6% versus 23% ( P=0.024), respectively. For patients with NIHSS 6 to 9 compared with the remaining DEFUSE 3 non-DAWN patients, thrombectomy trended toward a better chance of functional outcome (odds ratio, 1.86; CI, 0.36-9.529). Conclusions- Patients with pretreatment core infarct volumes <70 mL but too large for inclusion by DAWN criteria demonstrate benefit from endovascular therapy. More permissive pretreatment core thresholds in core-clinical mismatch selection paradigms may be appropriate. In contrast to data supporting a beneficial treatment effect across the full range of NIHSS scores in the entire DEFUSE 3 population, only a trend toward benefit of thrombectomy in patients with NIHSS 6 to 9 was found in this small subgroup.
Keywords: brain; brain ischemia; humans; standard of care; thrombectomy.
Figures
References
-
- Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016;387:1723–1731 - PubMed
-
- Leslie-Mazwi T, Chandra RV, Baxter BW, Arthur AS, Hussain MS, Singh IP, et al. Elvo: An operational definition. Journal of neurointerventional surgery 2018;10:507–509 - PubMed
-
- Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med 2018;378:11–21 - PubMed
-
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. 2018 guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the american heart association/american stroke association. Stroke 2018;49:e46–e110 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
