

Severe thoracic trauma caused left pneumonectomy complicated by right traumatic wet lung, reversed by extracorporeal membrane oxygenation support-a case report
- PMID: 30727998
- PMCID: PMC6366044
- DOI: 10.1186/s12890-019-0790-1
Severe thoracic trauma caused left pneumonectomy complicated by right traumatic wet lung, reversed by extracorporeal membrane oxygenation support-a case report
Abstract
Background: Double lumen intubation and one-lung ventilation should be applied without delay in cases of traumatic main bronchial rupture. In most cases, when the patients' vital signs have been stabilized, the repair can be performed. However, when one-lung ventilation is complicated by traumatic wet lung, the mortality rate is likely to be much higher.
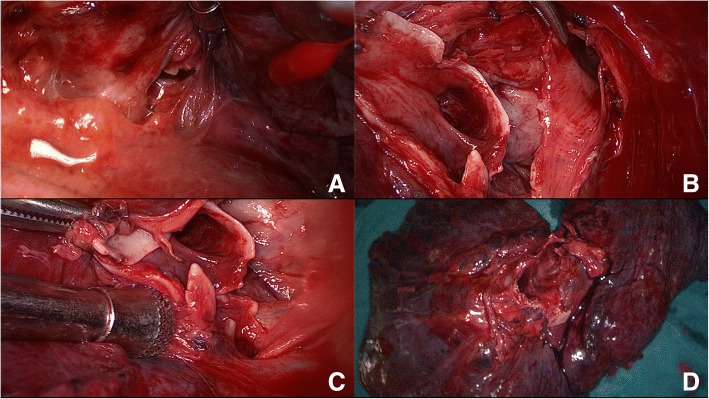
Case presentation: In this case, the patient experienced a left main bronchial rupture, bilateral traumatic wet lung, and acute respiratory distress syndrome (ARDS) because of severe thoracic trauma. Though the patient was treated with intubation and mechanical ventilation (MV), his oxygenation was still not stable. Thus, veno-venous extracorporeal membrane oxygenation (V-V ECMO) was initiated; upon improvement of oxygenation, the patient received an exploratory thoracotomy. Unfortunately, the rupture proved to be irreparable, resulting in a total left pneumonectomy. As there was severe ARDS caused by trauma, ECMO and ultra-low tidal volume (VT) MV strategy (3 ml/kg) were utilized for lung protection post-op. ECMO was sustained up to the 10th day, and MV until the 20th day, post-operation. With the support of MV, ECMO and other comprehensive measures, the patient made a recovery.
Conclusion: V-V ECMO and ultra-low VT MV helped this thoracic trauma patient survive the lung edema period and prevented ventilator associated pneumonia (VAP). In extreme situations, with the support of ECMO, the tidal volume may be lowered to 3 ml/kg.
Keywords: Acute respiratory distress syndrome; Extracorporeal membrane oxygenation; One lung ventilation; Thoracic trauma; Traumatic wet lung.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable (only standard care were performed).
Consent for publication
Patient gave consent for publication and consent for publication was written.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Haider T, Halat G, Heinz T, Hajdu S, Negrin LL. Thoracic trauma and acute respiratory distress syndrome in polytraumatized patients: a retrospective analysis. Minerva Anestesiol. 2017;83(10):1026–1033. - PubMed
-
- Karmy-Jones R, Jurkovich GJ, Shatz DV, Brundage S, Wall MJ, Jr, Engelhardt S, et al. Management of traumatic lung injury: a Western trauma association multicenter review. J Trauma. 2001;51(6):1049–1053. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
