

Porcine vs bovine surfactant therapy for preterm neonates with RDS: systematic review with biological plausibility and pragmatic meta-analysis of respiratory outcomes
- PMID: 30728009
- PMCID: PMC6366095
- DOI: 10.1186/s12931-019-0979-0
Porcine vs bovine surfactant therapy for preterm neonates with RDS: systematic review with biological plausibility and pragmatic meta-analysis of respiratory outcomes
Abstract
Background: Bovine surfactants are known to be clinically equivalent but it is unclear if porcine or bovine surfactants at their licensed dose should be preferred to treat respiratory distress syndrome in preterm neonates.
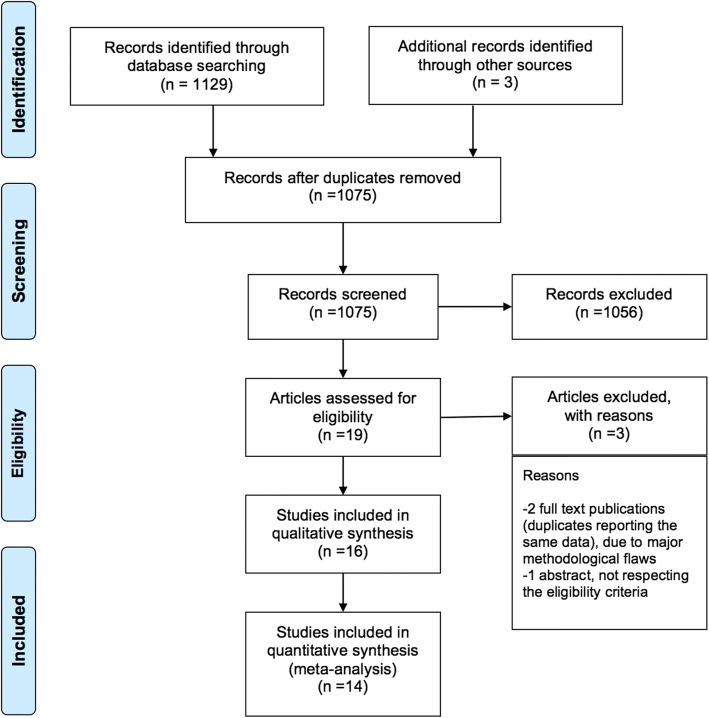
Methods: We performed a comprehensive review of biochemical and pharmacological features of surfactants to understand the biological plausibility of any clinical effect. We then performed a pragmatic meta-analysis comparing internationally marketed porcine and bovine surfactants for mortality and respiratory outcomes. Search for randomised controlled trials with no language/year restrictions and excluding "grey" literature, unpublished or non-peer reviewed reports was conducted, following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and the most recent methodological recommendations.
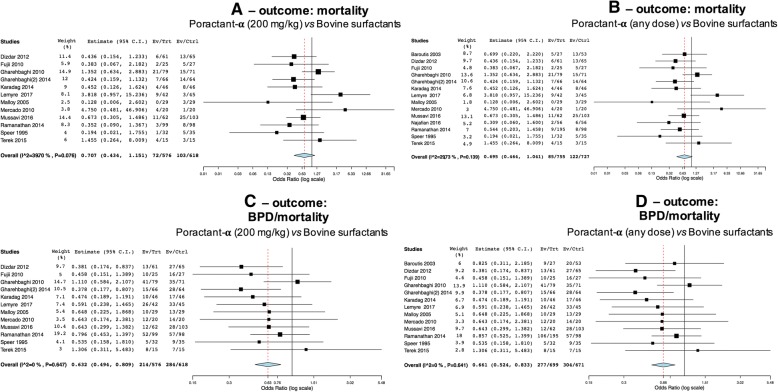
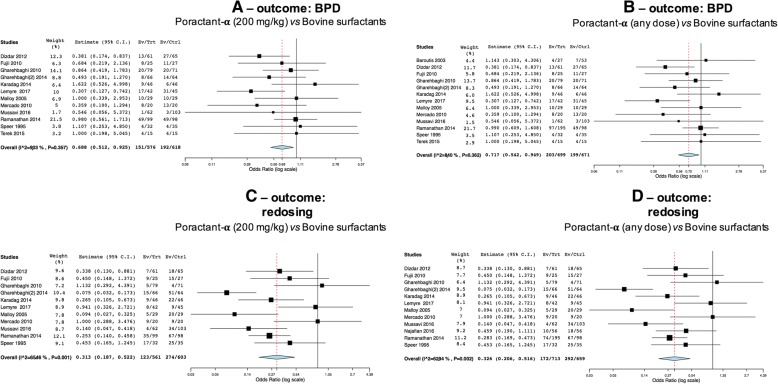
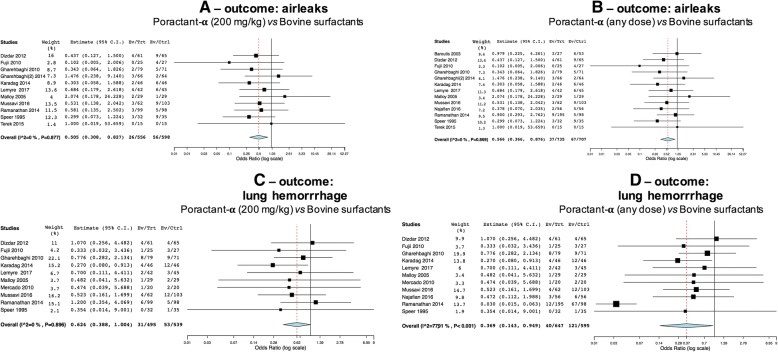
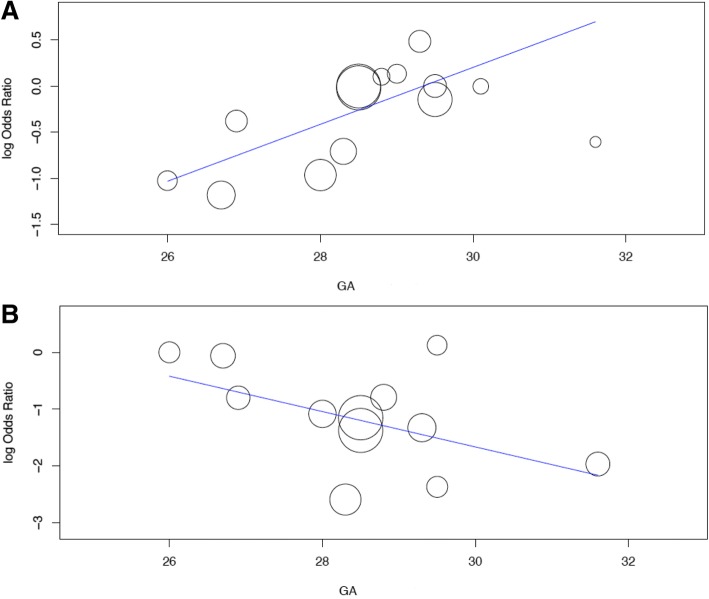
Results: Sixteen articles were included in the review and 14 in the meta-analysis (1491 neonates). 200 mg/kg poractant-α (a porcine surfactant) was associated with lower BPD/mortality (OR 0.632[95%CI:0.494, 0.809];p < 0.001),BPD (OR 0.688[95%CI:0.512, 0.925];p = 0.013), retreatment (OR 0.313[95%CI:0.187, 0.522];p < 0.0001), airleaks (OR 0.505[95%CI:0.308, 0.827];p = 0.006) and lung haemorrhage (OR 0.624[95%CI:0.388, 1];p = 0.051). Gestational age is associated with effect size for BPD (coefficient: 0.308 [95%CI:0.063, 0.554];p = 0.014) and surfactant retreatment (coefficient: -0.311 [95%CI:-0.595, - 0.028];p = 0.031).
Conclusion: 200 mg/kg poractant-α is associated with better respiratory outcomes compared to bovine surfactants at their licensed dose. The effect of poractant-α on BPD and surfactant retreatment is greater at lowest and highest gestational ages, respectively.
Trial registration: PROSPERO n.42017075251 .
Keywords: Neonate; RDS; Surfactant; Therapy.
Conflict of interest statement
Ethics approval
Not applicable as this is a review and meta-analysis. Trials meta-analysed have all received their original ethical approval.
Consent for publication
Not applicable
Competing interests
A/Prof. D. De Luca has received grants for research and educational projects from Chiesi Pharmaceuticals spa and ABBVIE inc. He also received travel grants from ABBVIE inc. He served as consultant and lecturer for both Chiesi Pharmaceuticals spa and ABBVIE inc. Finally, he has been member of the external advisory board for both Chiesi Pharmaceuticals spa and ABBVIE inc. These companies produce two surfactants analysed in the paper, but they had no role in design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, approval of the manuscript or decision to submit it for publication. The other authors declare no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Boghossian NS, Geraci M, Edwards EM, et al. Morbidity and Mortality in Small for Gestational Age Infants at 22 to 29 Weeks' Gestation. Pediatrics. 2018;141(2). 10.1542/peds.2017-2533. - PubMed
-
- Subramaniam P, Ho JJ, Davis PG. Prophylactic nasal continuous positive airway pressure for preventing morbidity and mortality in very preterm infants. Cochrane Database Syst Rev. 2016;6:CD001243. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
