

Operative volume and surgical case distribution in Uganda's public sector: a stratified randomized evaluation of nationwide surgical capacity
- PMID: 30728037
- PMCID: PMC6366061
- DOI: 10.1186/s12913-019-3920-9
Operative volume and surgical case distribution in Uganda's public sector: a stratified randomized evaluation of nationwide surgical capacity
Abstract
Background: Little is known about operative volume, distribution of cases, or capacity of the public sector to deliver essential surgical services in Uganda.
Methods: A standardized mixed-methods surgical assessment and retrospective operative logbook review were completed at 16 randomly selected public hospitals serving 64·0% of Uganda's population.
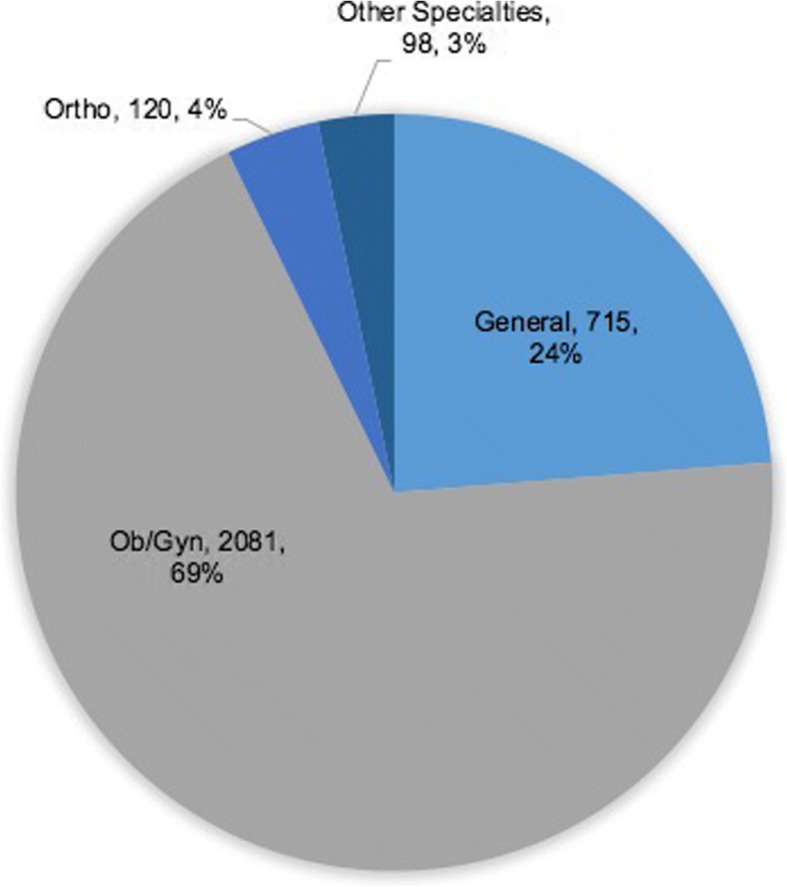
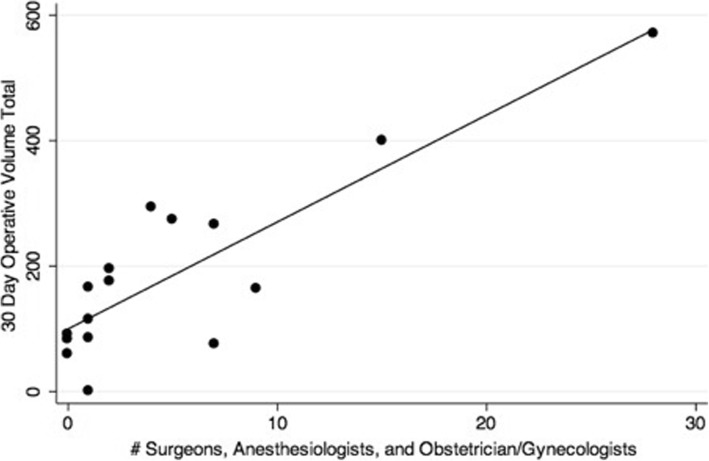
Results: A total of 3014 operations were recorded, annualizing to a surgical volume of 36,670 cases/year or 144·5 operations/100,000people/year. Absolute surgical volume was greater at regional referral than general hospitals (p < 0·001); but, relative surgical volume/catchment population was greater at the general versus regional level (p = 0·03). Most patients undergoing operations were women (78·3%) with a mean age of 26·9 years. The overall case distribution was 69·0% obstetrics/gynecology, 23·7% general surgery, 4·0% orthopedics, and 3·3% other subspecialties. Cesarean sections were the most common operation (55·8%). Monthly operative volume was strongly predicted by number of surgical, anesthetic, and obstetric physician providers (훽=10·72, p = 0·005, R2 = 0·94) when controlling for confounders. Notably, operative volume was not correlated with availability of electricity, oxygen, light source, suction, blood, instruments, suture, gloves, intravenous fluid, or antibiotics.
Conclusion: An understanding of operative case volume and distribution is essential in facilitating targeted interventions to strengthen surgical capacity. These data suggest that surgical workforce is the critical driver of operative volume in the Ugandan public sector. Investment in the surgical workforce is imperative to ensure access to safe, timely, and affordable surgical and anaesthesia care.
Keywords: Case distribution; Global surgery; Operative volume; Surgical workforce; Uganda.
Conflict of interest statement
Ethics approval and consent to participate
The institutional review board (IRB) at Children’s Hospital Boston deemed this study exempt. The IRB at Mbarara University of Science and Technology and the Uganda National Council for Science and Technology approved this study. Permission and verbal informed consent to participate was additionally obtained from each facility participating in the assessment. Verbal informed consent was deemed sufficient given the IRB exemption and the fact that no identifying information was collected from study participants. Permission was obtained from each facility to access surgical logbooks. All operative logbook data were kept in a secure location and immediately de-identified.
Consent for publication
N/A
Competing interests
The authors declare that they have no competing interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
