

Radiological diagnosis of brain radiation necrosis after cranial irradiation for brain tumor: a systematic review
- PMID: 30728041
- PMCID: PMC6364413
- DOI: 10.1186/s13014-019-1228-x
Radiological diagnosis of brain radiation necrosis after cranial irradiation for brain tumor: a systematic review
Abstract
Introduction: This systematic review aims to elucidate the diagnostic accuracy of radiological examinations to distinguish between brain radiation necrosis (BRN) and tumor progression (TP).
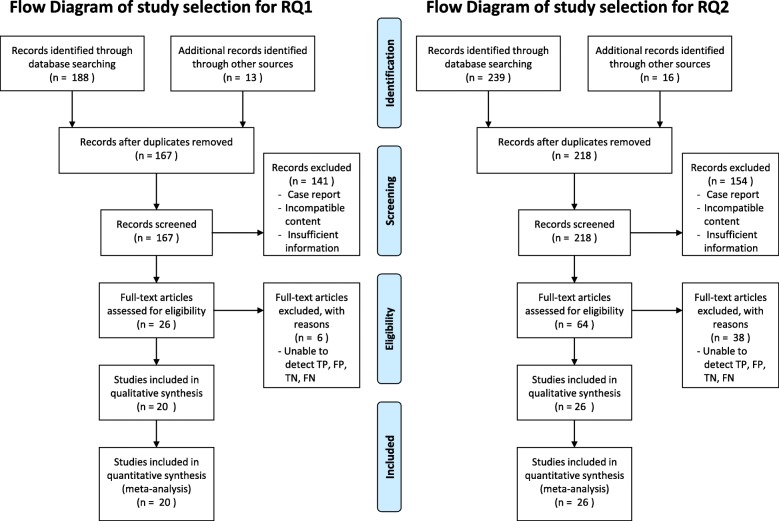
Methods: We divided diagnostic approaches into two categories as follows-conventional radiological imaging [computed tomography (CT) and magnetic resonance imaging (MRI): review question (RQ) 1] and nuclear medicine studies [single photon emission CT (SPECT) and positron emission tomography (PET): RQ2]-and queried. Our librarians conducted a comprehensive systematic search on PubMed, the Cochrane Library, and the Japan Medical Abstracts Society up to March 2015. We estimated summary statistics using the bivariate random effects model and performed subanalysis by dividing into tumor types-gliomas and metastatic brain tumors.
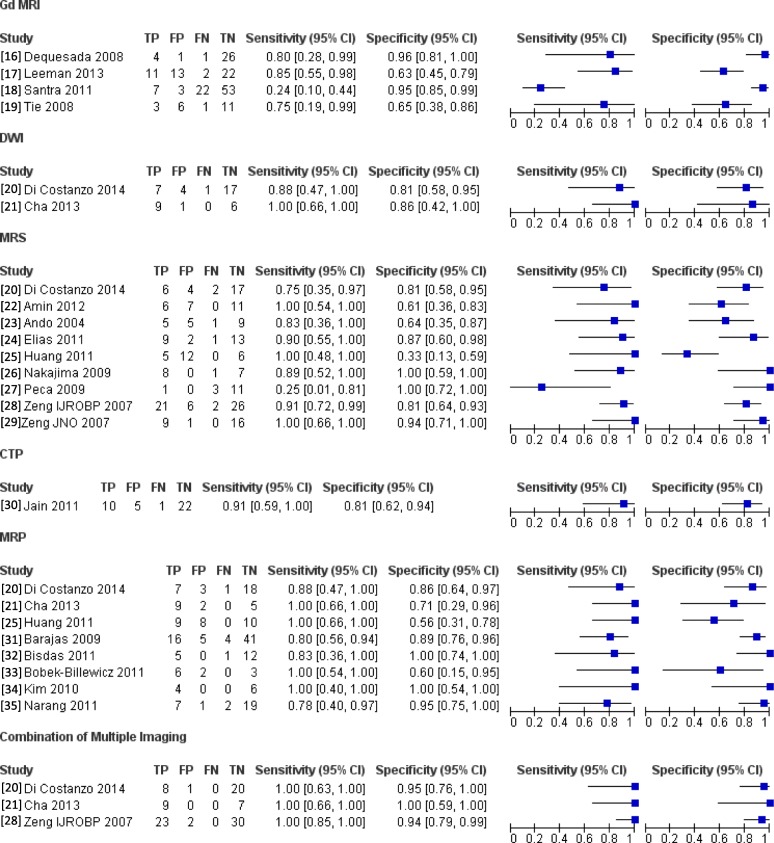
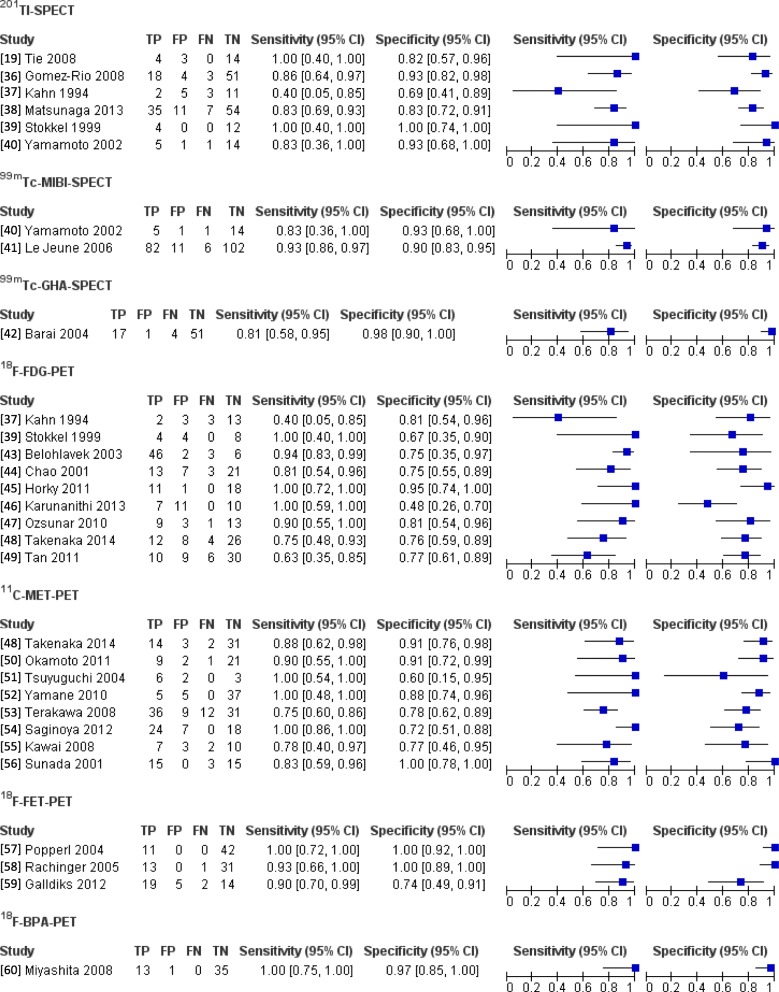
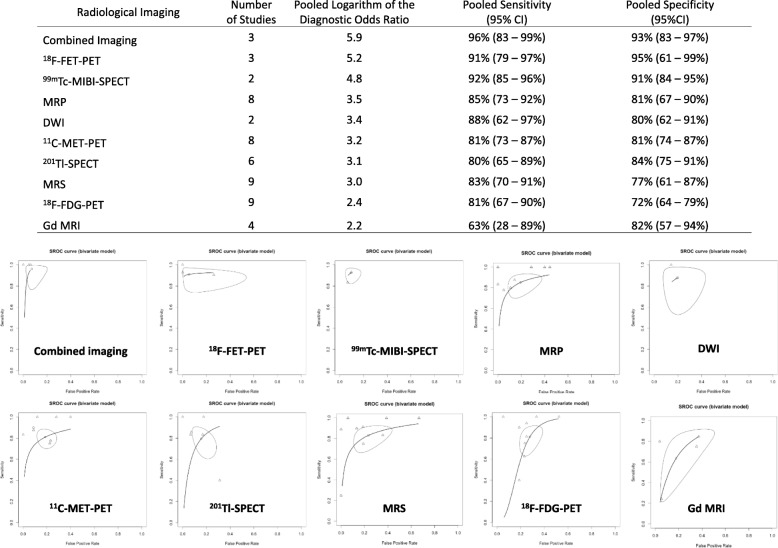
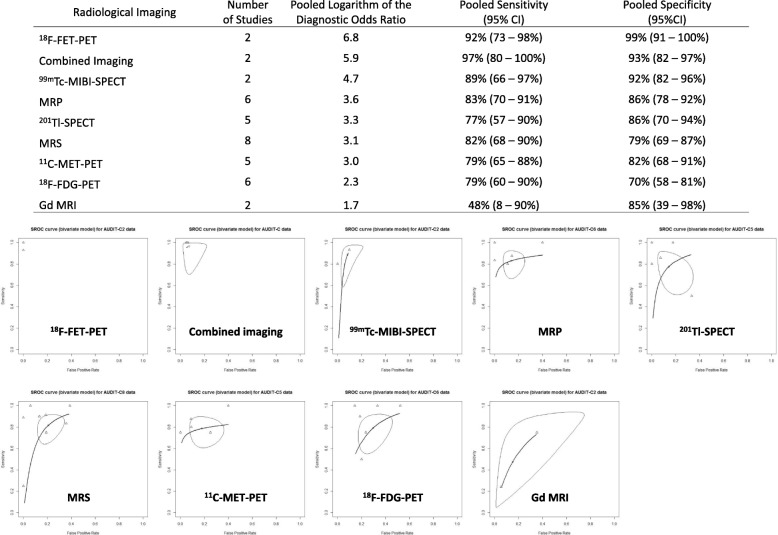
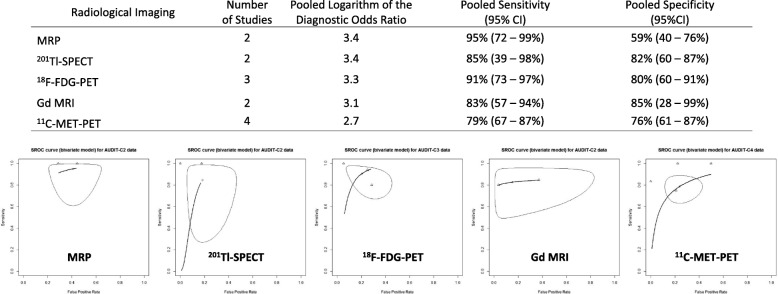
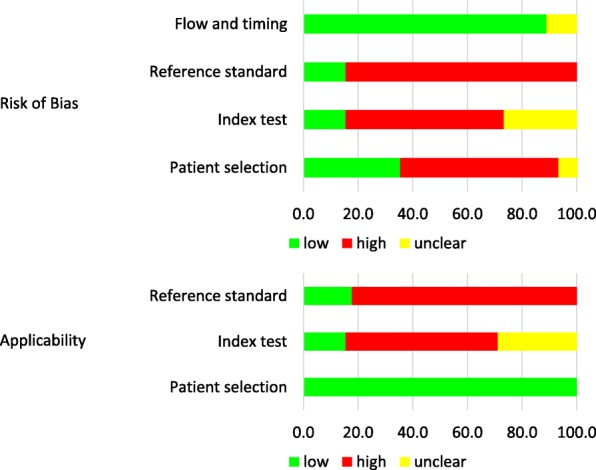
Results: Of 188 and 239 records extracted from the database, we included 20 and 26 studies in the analysis for RQ1 and RQ2, respectively. In RQ1, we used gadolinium (Gd)-enhanced MRI, diffusion-weighted image, MR spectroscopy, and perfusion CT/MRI to diagnose BRN in RQ1. In RQ2, 201Tl-, 99mTc-MIBI-, and 99mTc-GHA-SPECT, and 18F-FDG-, 11C-MET-, 18F-FET-, and 18F-BPA-PET were used. In meta-analysis, Gd-enhanced MRI exhibited the lowest sensitivity [63%; 95% confidence interval (CI): 28-89%] and diagnostic odds ratio (DOR), and combined multiple imaging studies displayed the highest sensitivity (96%; 95% CI: 83-99%) and DOR among all imaging studies. In subanalysis for gliomas, Gd-enhanced MRI and 18F-FDG-PET revealed low DOR. Conversely, we observed no difference in DOR among radiological imaging in metastatic brain tumors. However, diagnostic parameters and study subjects often differed among the same imaging studies. All studies enrolled a small number of patients, and only 10 were prospective studies without randomization.
Conclusions: Differentiating BRN from TP using Gd-enhanced MRI and 18F-FDG-PET is challenging for patients with glioma. Conversely, BRN could be diagnosed by any radiological imaging in metastatic brain tumors. This review suggests that combined multiparametric imaging, including lesional metabolism and blood flow, could enhance diagnostic accuracy, compared with a single imaging study. Nevertheless, a substantial risk of bias and indirectness of reviewed studies hindered drawing firm conclusion about the best imaging technique for diagnosing BRN.
Keywords: Brain tumor; Diagnosis; Radiation necrosis; Radiology; Recurrence.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Nordal RA, Nagy A, Pintilie M, Wong CS. Hypoxia and hypoxia-inducible factor-1 target genes in central nervous system radiation injury: a role for vascular endothelial growth factor. Clin Cancer Res. 2004;10:3342–3353. - PubMed
-
- Kureshi SA, Hofman FM, Schneider JH, Chin LS, Apuzzo ML, Hinton DR. Cytokine expression in radiation-induced delayed cerebral injury. Neurosurgery. 1994;35:822–829. - PubMed
-
- Nonoguchi N, Miyatake S, Fukumoto M, Furuse M, Hiramatsu R, Kawabata S, Kuroiwa T, Tsuji M, Ono K. The distribution of vascular endothelial growth factor-producing cells in clinical radiation necrosis of the brain: pathological consideration of their potential roles. J Neuro-Oncol. 2011;105:423–431. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
