

Hemodynamic variables in aneurysms are associated with thrombotic risk in children with Kawasaki disease
- PMID: 30728104
- PMCID: PMC6511338
- DOI: 10.1016/j.ijcard.2019.01.092
Hemodynamic variables in aneurysms are associated with thrombotic risk in children with Kawasaki disease
Abstract
Background: Thrombosis is a major adverse outcome associated with coronary artery aneurysms (CAAs) resulting from Kawasaki disease (KD). Clinical guidelines recommend initiation of anticoagulation therapy with maximum CAA diameter (Dmax) ≥8 mm or Z-score ≥ 10. Here, we investigate the role of aneurysm hemodynamics as a superior method for thrombotic risk stratification in KD patients.
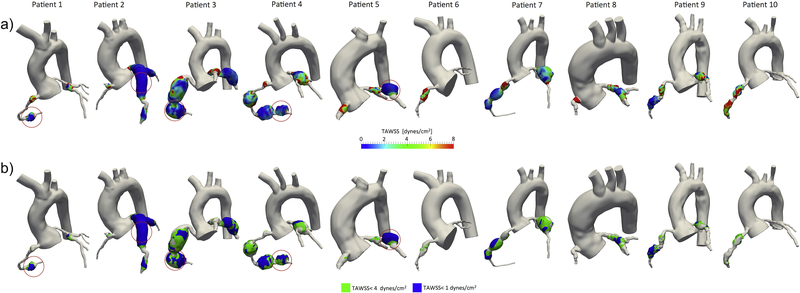
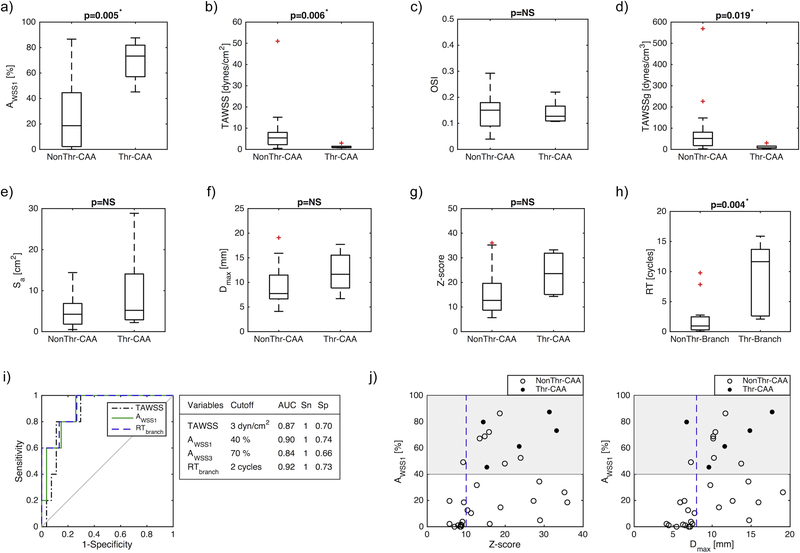
Methods and results: We retrospectively studied ten KD patients with CAAs, including five patients who developed thrombosis. We constructed patient-specific anatomic models from cardiac magnetic resonance images and performed computational hemodynamic simulations using SimVascular. Our simulations incorporated pulsatile flow, deformable arterial walls and boundary conditions automatically tuned to match patient-specific arterial pressure and cardiac output. From simulation results, we derived local hemodynamic variables including time-averaged wall shear stress (TAWSS), low wall shear stress exposure, and oscillatory shear index (OSI). Local TAWSS was significantly lower in CAAs that developed thrombosis (1.2 ± 0.94 vs. 7.28 ± 9.77 dynes/cm2, p = 0.006) and the fraction of CAA surface area exposed to low wall shear stress was larger (0.69 ± 0.17 vs. 0.25 ± 0.26%, p = 0.005). Similarly, longer residence times were obtained in branches where thrombosis was confirmed (9.07 ± 6.26 vs. 2.05 ± 2.91 cycles, p = 0.004). No significant differences were found for OSI or anatomical measurements such us Dmax and Z-score. Assessment of thrombotic risk according to hemodynamic variables had higher sensitivity and specificity compared to standard clinical metrics (Dmax, Z-score).
Conclusions: Hemodynamic variables can be obtained non-invasively via simulation and may provide improved thrombotic risk stratification compared to current diameter-based metrics, facilitating long-term clinical management of KD patients with persistent CAAs.
Keywords: Aneurysm; Computational modeling; Hemodynamics; Kawasaki disease; Magnetic resonance imaging; Thrombosis.
Copyright © 2019 Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
References
-
- McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals From the American Heart Association. Circulation. 2017;135:e927–e99. - PubMed
-
- Bluestein D, Niu L, Schoephoerster RT, Dewanjee MK. Fluid mechanics of arterial stenosis: relationship to the development of mural thrombus. Ann Biomed Eng. 1997;25:344–56. - PubMed
-
- Di Achille P, Tellides G, Figueroa CA, Humphrey JD. A haemodynamic predictor of intraluminal thrombus formation in abdominal aortic aneurysms. Proceedings of the Royal Society A: Mathematical, Physical and Engineering Science. 2014;470.
-
- Bluestein D, Niu L, Schoephoerster RT, Dewanjee MK. Steady flow in an aneurysm model: correlation between fluid dynamics and blood platelet deposition. J Biomech Eng. 1996;118:280–6. - PubMed
