

Noninvasive Arterial Testing: What and When to Use
- PMID: 30728654
- PMCID: PMC6363559
- DOI: 10.1055/s-0038-1676328
Noninvasive Arterial Testing: What and When to Use
Abstract
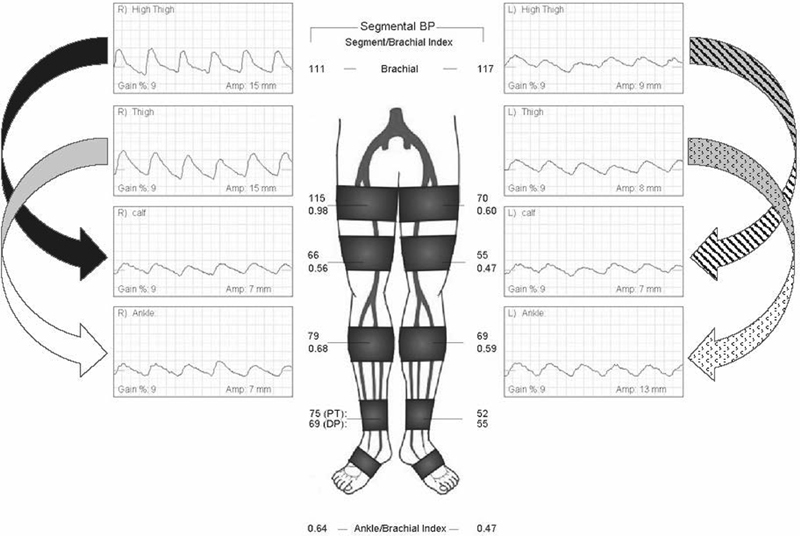
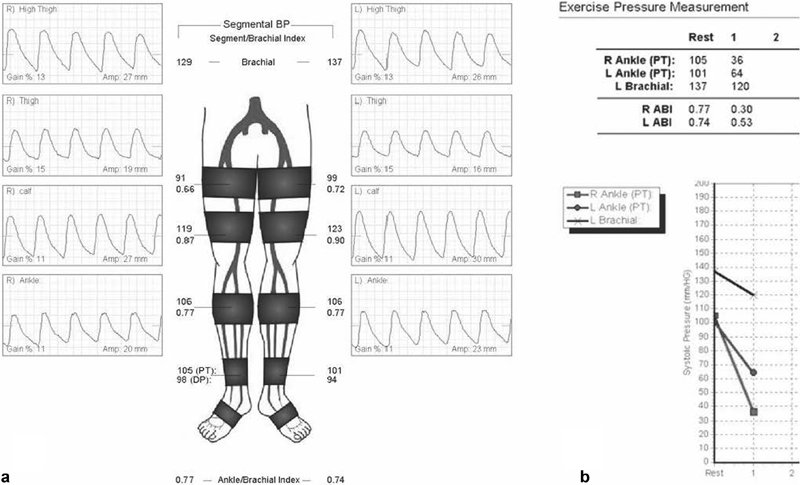
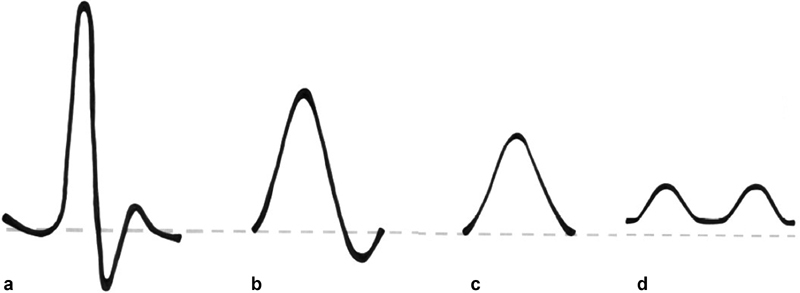
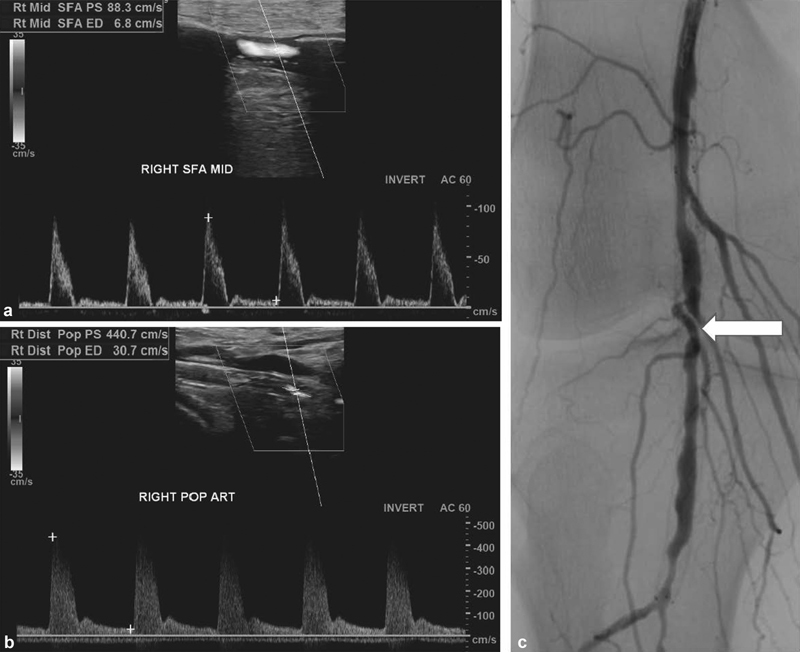
Peripheral arterial disease (PAD) represents a growing public health issue that continues to be underdiagnosed. In its most severe form, critical limb ischemia, it contributes to expanding morbidity with minor and major limb amputations. PAD is strongly associated with increased mortality, as it is known to be concomitant with coronary and cerebrovascular disease. Diagnosis of PAD relies on noninvasive arterial testing, a class of tests that can provide physiologic or morphologic information. Physiologic tests such as ankle-brachial index, toe-brachial index, pulse volume recordings, and arterial duplex evaluation are the mainstay of gateway evaluation and surveillance. Morphologic exams such as computer tomographic angiography and magnetic resonance angiography are appropriate for preprocedural anatomic evaluation in patients with established vascular disease. This review focuses on physiologic exams.
Keywords: ankle-brachial index; interventional radiology; noninvasive arterial testing; physiologic arterial test; pulse volume recordings.
Figures
References
-
- Nehler M R, Duval S, Diao L et al. Epidemiology of peripheral arterial disease and critical limb ischemia in an insured national population. J Vasc Surg. 2014;60(03):686–9500. - PubMed
-
- Fowkes F G, Rudan D, Rudan Iet al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis Lancet 2013382(9901):1329–1340. - PubMed
-
- McCann T E, Scoutt L M, Gunabushanam G. A practical approach to interpreting lower extremity noninvasive physiologic studies. Radiol Clin North Am. 2014;52(06):1343–1357. - PubMed
-
- Del Conde I, Benenati J F. Noninvasive testing in peripheral arterial disease. Interv Cardiol Clin. 2014;3(04):469–478. - PubMed
