

Naringenin Attenuates Myocardial Ischemia-Reperfusion Injury via cGMP-PKGI α Signaling and In Vivo and In Vitro Studies
- PMID: 30728891
- PMCID: PMC6341255
- DOI: 10.1155/2019/7670854
Naringenin Attenuates Myocardial Ischemia-Reperfusion Injury via cGMP-PKGI α Signaling and In Vivo and In Vitro Studies
Abstract
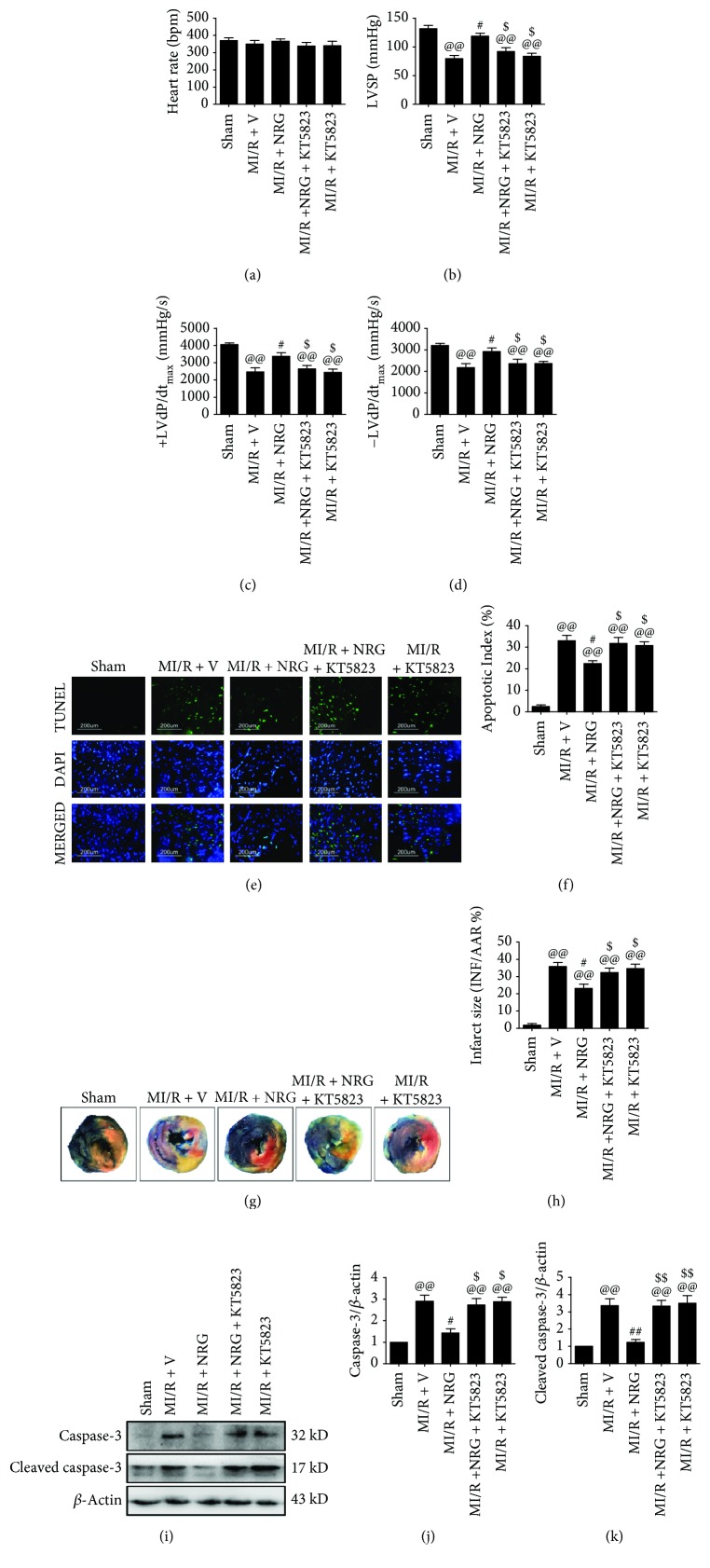
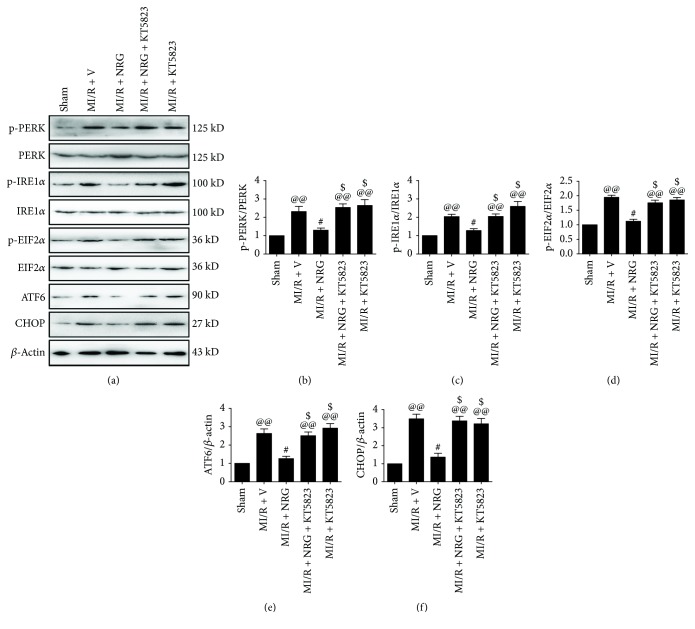
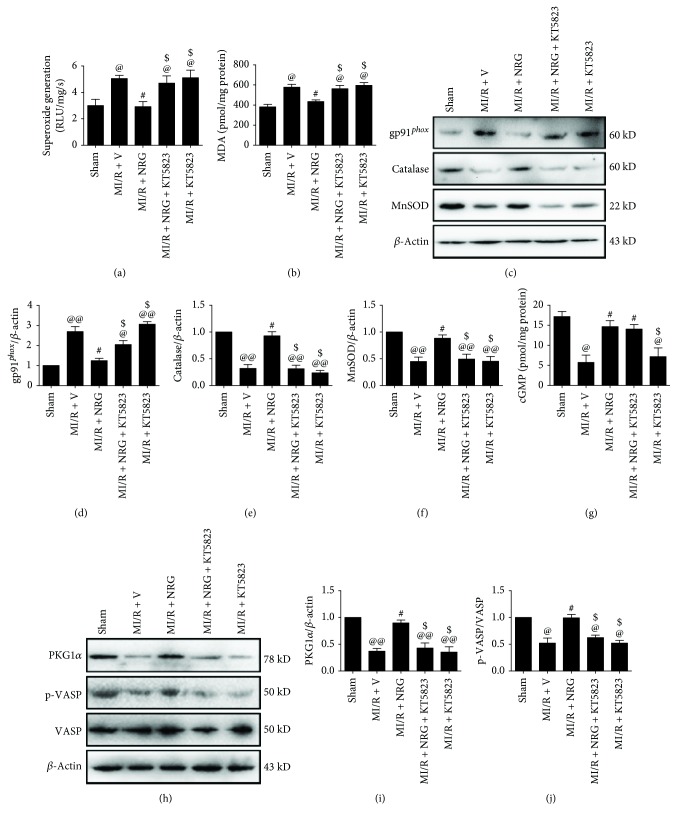
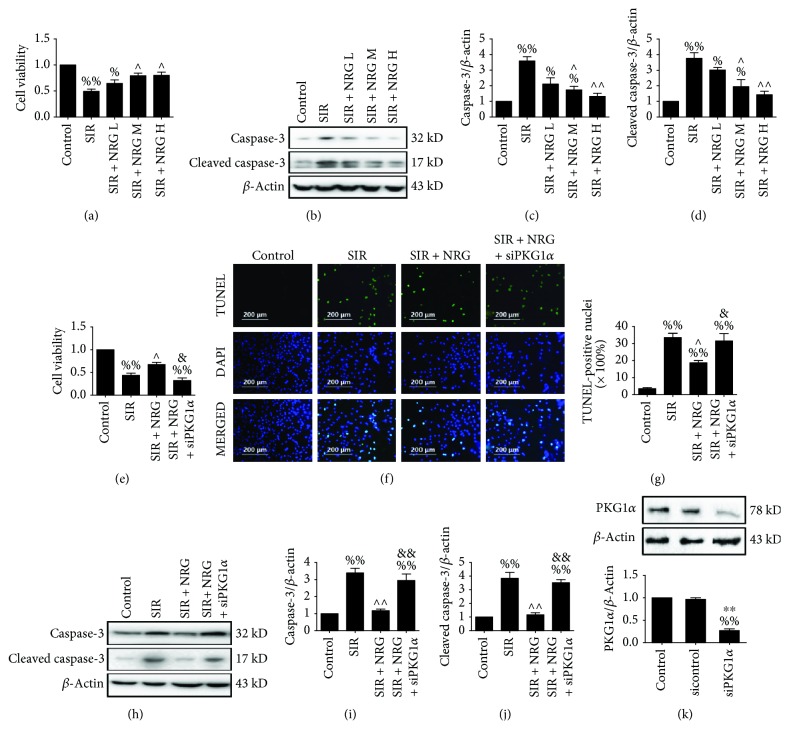
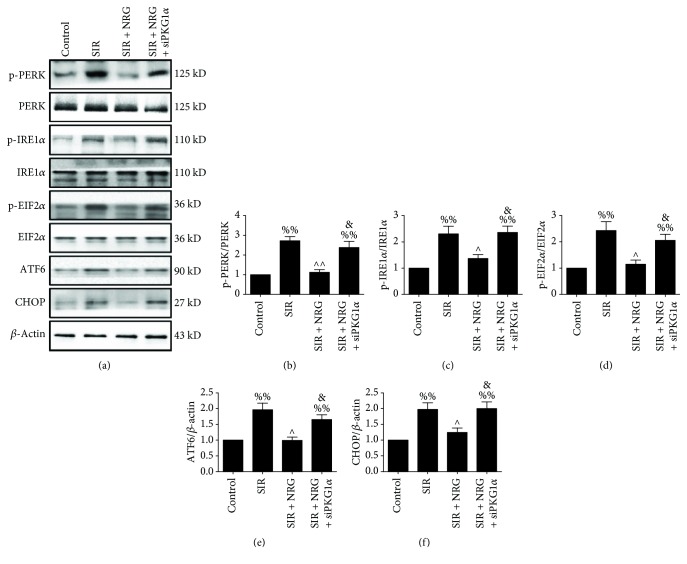
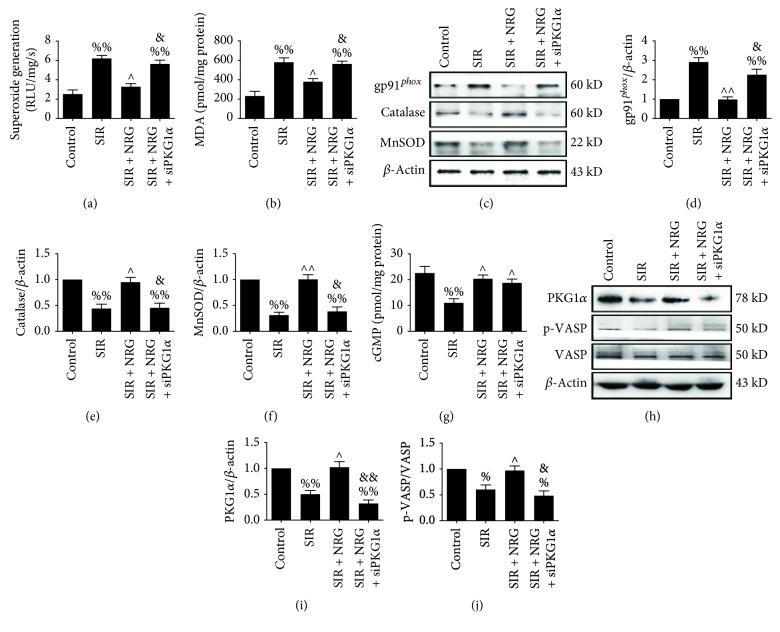
Endoplasmic reticulum (ER) stress and oxidative stress contribute greatly to myocardial ischemia-reperfusion (MI/R) injury. Naringenin, a flavonoid derived from the citrus genus, exerts cardioprotective effects. However, the effects of naringenin on ER stress as well as oxidative stress under MI/R condition and the detailed mechanisms remain poorly defined. This study investigated the protective effect of naringenin on MI/R-injured heart with a focus on cyclic guanosine monophosphate- (cGMP-) dependent protein kinase (PKG) signaling. Sprague-Dawley rats were treated with naringenin (50 mg/kg/d) and subjected to MI/R surgery with or without KT5823 (2 mg/kg, a selective inhibitor of PKG) cotreatment. Cellular experiment was conducted on H9c2 cardiomyoblasts subjected to simulated ischemia-reperfusion treatment. Before the treatment, the cells were incubated with naringenin (80 μmol/L). PKGIα siRNA was employed to inhibit PKG signaling. Our in vivo and in vitro data showed that naringenin effectively improved heart function while it attenuated myocardial apoptosis and infarction. Furthermore, pretreatment with naringenin suppressed MI/R-induced oxidative stress as well as ER stress as evidenced by decreased superoxide generation, myocardial MDA level, gp91 phox expression, and phosphorylation of PERK, IRE1α, and EIF2α as well as reduced ATF6 and CHOP. Importantly, naringenin significantly activated myocardial cGMP-PKGIα signaling while inhibition of PKG signaling with KT5823 (in vivo) or siRNA (in vitro) not only abolished these actions but also blunted naringenin's inhibitory effects against oxidative stress and ER stress. In summary, our study demonstrates that naringenin treatment protects against MI/R injury by reducing oxidative stress and ER stress via cGMP-PKGIα signaling. Its cardioprotective effect deserves further clinical study.
Figures
References
-
- Hausenloy D. J., Garcia-Dorado D., Botker H. E., et al. Novel targets and future strategies for acute cardioprotection: Position Paper of the European Society of Cardiology Working Group on Cellular Biology of the Heart. Cardiovascular Research. 2017;113(6):564–585. doi: 10.1093/cvr/cvx049. - DOI - PubMed
-
- Perrino C., Barabasi A. L., Condorelli G., et al. Epigenomic and transcriptomic approaches in the post-genomic era: path to novel targets for diagnosis and therapy of the ischaemic heart? Position Paper of the European Society of Cardiology Working Group on Cellular Biology of the Heart. Cardiovascular Research. 2017;113(7):725–736. doi: 10.1093/cvr/cvx070. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
