

Case Reports
doi: 10.1155/2019/9454201.
eCollection 2019.
A Case Series of Breast Metastases from Different Extramammary Malignancies and Their Literature Review
Affiliations
- PMID: 30729058
- PMCID: PMC6341250
- DOI: 10.1155/2019/9454201
Item in Clipboard
Case Reports
A Case Series of Breast Metastases from Different Extramammary Malignancies and Their Literature Review
Case Rep Radiol.
.
Abstract
Metastasis to the breast from all other primary sites is unusual. Twelve patients were diagnosed between 2007 and 2017 at National Cancer Institute, Mexico. Solitary or multiple masses, round or oval, and hypoechoic and solid lesions with posterior acoustic shadowing were patterns commonly reported in these patients; other arrangements include diffuse involvement of the breast simulating an inflammatory carcinoma. The development of a breast metastasis is revealed, in our experience, as a negative prognostic factor. Thus, the radiologist should know about the varied appearance of metastatic breast lesions and provide radiopathological correlations when available.
Figures
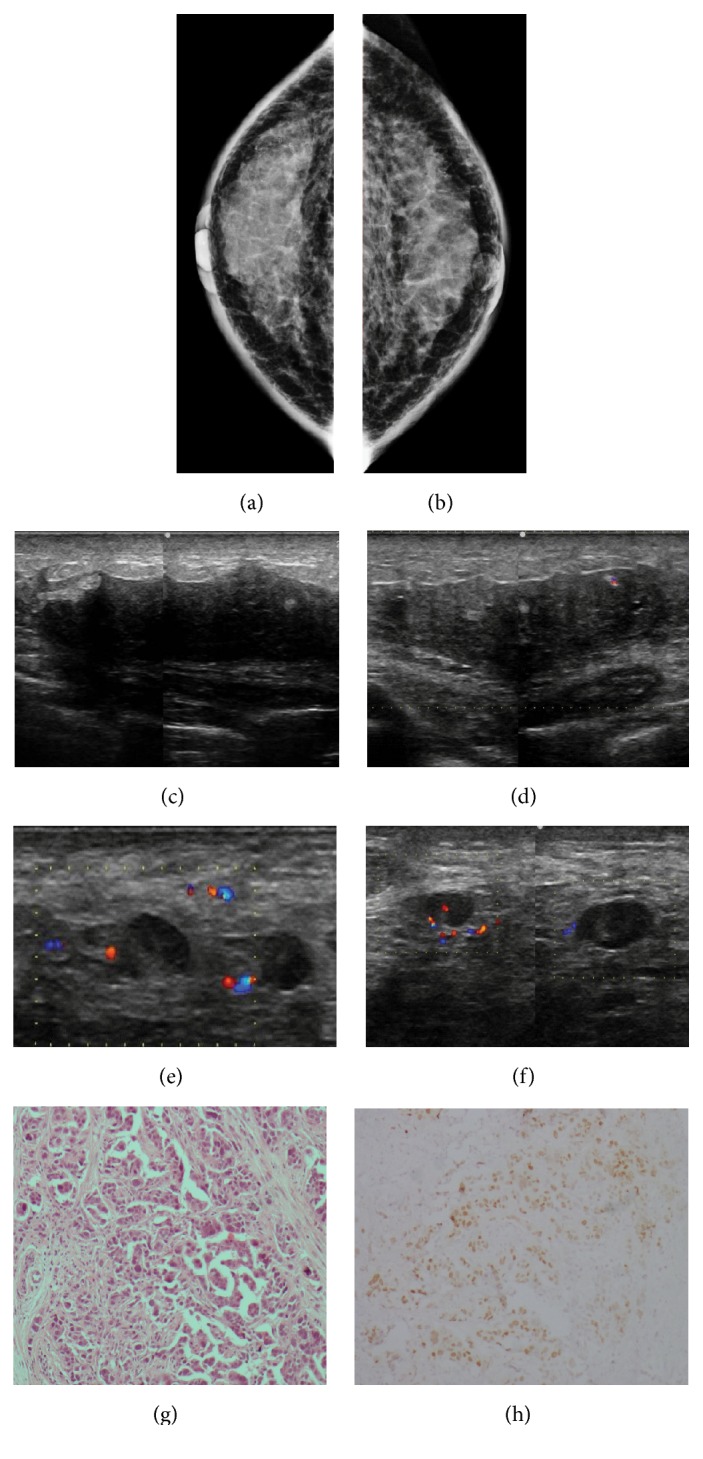
Case
1. A 66-year-old-woman diagnosed with primary ovarian carcinoma with signet ring cells. On initial presentation, the patient showed breast lymphedema. Mammogram revealed abnormal skin enhancement, thickening, and edema consistent with inflammatory changes (a–b). Breast sonography exposed architectural distortions with a posterior combined pattern (c–d). Bilateral axillary lymph nodes with irregular cortical thickening were also found (e–f). Metastatic signet ring cell carcinoma to the breast was confirmed following a histopathological analysis of the breast and lymph node specimens. HE staining and immunohistochemistry analysis of the metastases. HE staining revealed the malignant cells in the breast tumor (g), and the immunohistochemistry analysis indicated that the cells were positive for PAX8 (h).
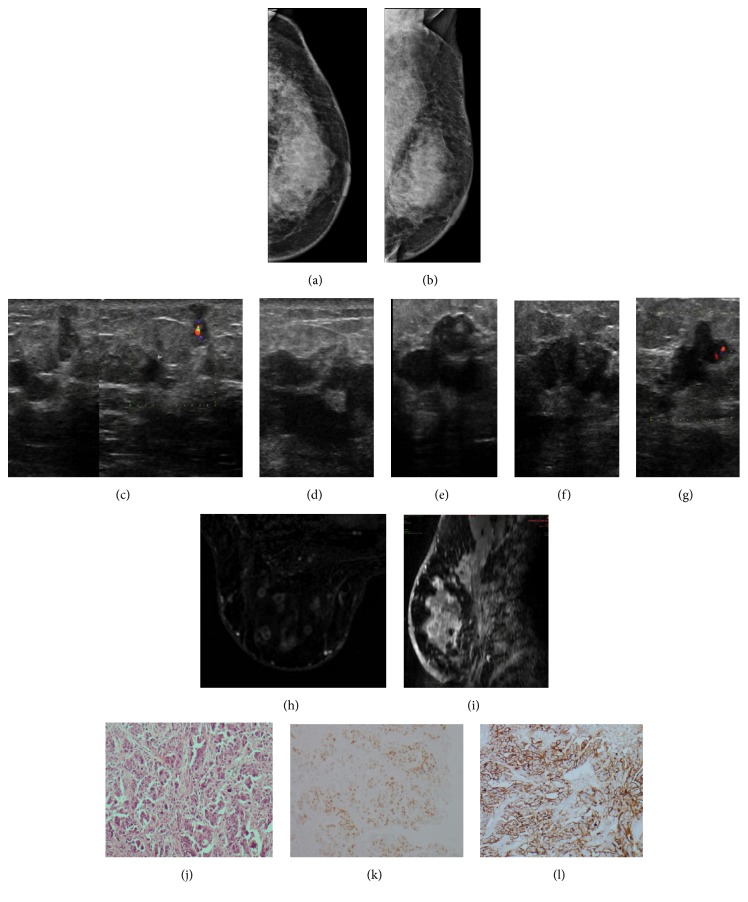
Case
2. A 60-year-old woman diagnosed with papillary serous ovarian carcinoma. A palpable mass in the left breast was noticed by the patient 2 years after initial diagnosis. Mammogram revealed dermal thickening and diffusely increased breast density (a–b). A distortion was evident in the breast tail as well, indicating skin retraction (b). Grayscale and Doppler ultrasound showed bilateral hypoechoic irregular masses with angular margins. A nonparallel orientation and central vascularity were observed in some masses. Multifocal and diffuse distribution of the lesions was noted on ultrasound (c–g). Similarly, subtracted images from magnetic resonance demonstrated multiple irregular masses with circumscribed margins and rim enhancement (h). Conglomerate lesions infiltrating the major pectoralis muscle were also exposed (i). HE staining and immunohistochemistry analysis of the metastases. HE staining revealed the malignant cells in the breast tumor (j), and the immunohistochemistry analysis indicated that the cells were positive for PAX8 (k) and CA125 (l).

Case
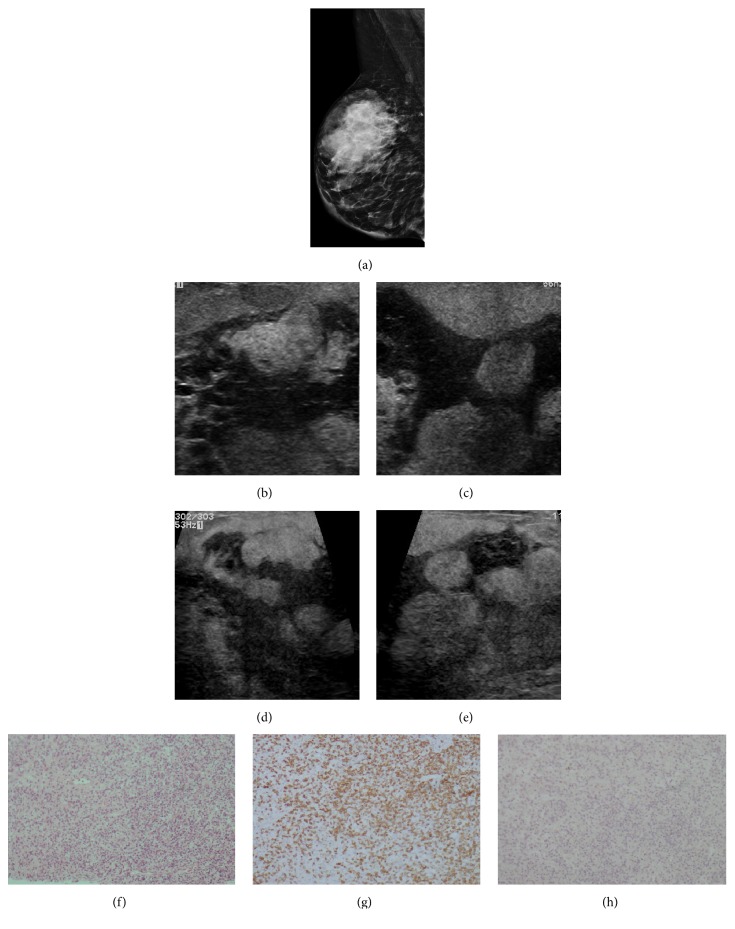
3. A 41-year-old woman diagnosed with a low-differentiated carcinoma. Contrast-enhanced computed tomography (CT) scan demonstrated an incidental finding consistent with a mass on the right breast (a). Although this lesion was palpable, it was not detectable on mammography (b). Then, an ultrasound was performed, showing an oval mass with parallel orientation, indistinct margins, a heterogeneous echo pattern, and posterior acoustic enhancement (c–d). HE staining and immunohistochemistry analysis of the metastases. HE staining revealed the malignant cells in the breast tumor (e), and the immunohistochemistry analysis indicated that the cells were positive for PAX8 (f) and WT4 (g).
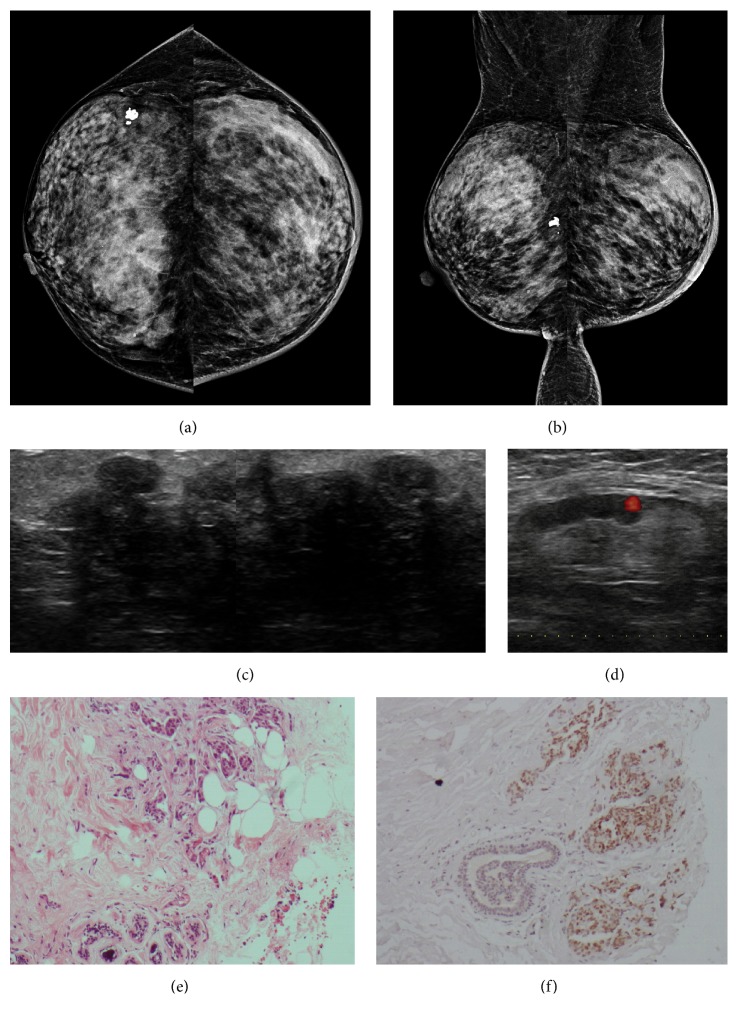
Case
4. A 56-year-old woman diagnosed with ovarian adenocarcinoma. One month after diagnosis, the patient presented with palpable axillary adenopathy. Mammogram showed dermal and trabecular thickening in the left breast, with diffusely increased density of the mammary tissue (a–b). On ultrasound, an irregular hypoechoic mass with indistinct margins was revealed (c). An axillary lymph node with cortical indentation was also observed by ultrasound (d). HE staining and immunohistochemistry analysis of the metastases. HE staining revealed the malignant cells in the breast tumor (e), and the immunohistochemistry analysis indicated that the cells were positive for PAX8 (f).

Case
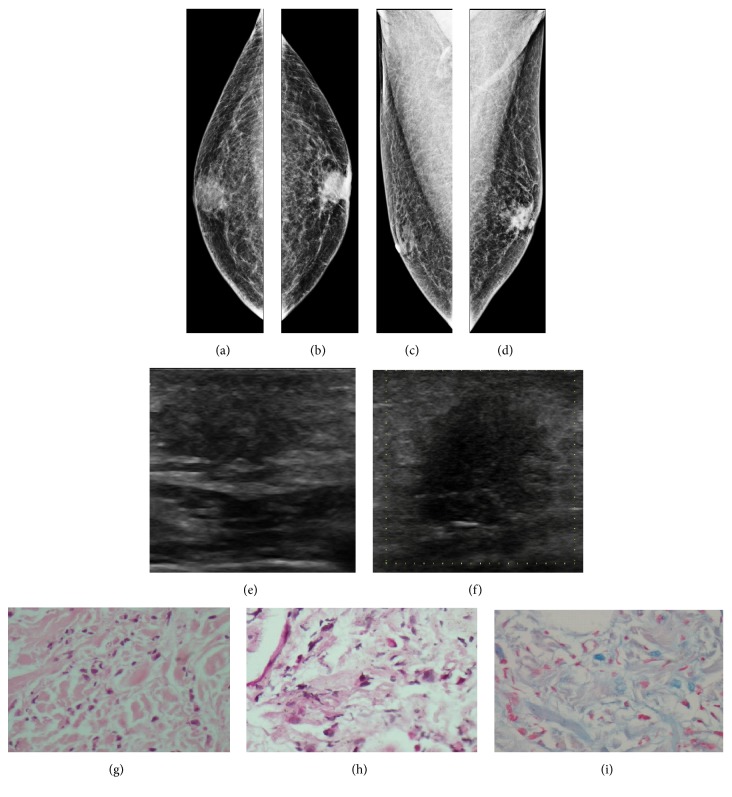
5. A 45-year-old woman with metastatic melanoma that presented as an isolated breast tumor. Upon interrogation, the patient reported a 1-month history of migraine and attacks of vertigo. Magnetic resonance imaging showed multiple heterogeneous enhancing masses suggesting the presence of metastatic disease (a). Intracranial hemorrhage focus was corroborated by fluid–fluid levels on gradient-echo imaging (b). Following the suspicion of metastatic disease, mammography was performed, demonstrating a subtle increase in density in both breasts (c–d). On ultrasound, an oval, hypoechoic mass with multilobulated margins was shown in the left breast (e). HE staining and immunohistochemistry analysis of the metastases. HE staining revealed the malignant cells in the breast tumor (f), and the immunohistochemistry analysis indicated that the cells were positive for melan-A (g).
Case
6. A 20-year-old woman with nodular melanoma. The patient presented with a 9-month history of nevus in the neck around the middle line. The woman was lost to follow-up before surgery, and 10 months later, she returned with a palpable mass in the right breast. Mammogram showed an oval mass with circumscribed margins (a–b). Ultrasound images demonstrated a sizeable oval mass with a parallel orientation, circumscribed margins, and absent posterior acoustic findings (c). A lymph node with irregular cortical enhancement was also exhibited (d). HE staining and immunohistochemistry analysis of the metastases. HE staining revealed the malignant cells in the breast tumor (e), and the immunohistochemistry analysis indicated that the cells were positive for HMB45 (f).
Case
7. A 71-year-old woman with malignant melanoma. Two years after diagnosis, the patient presented with a palpable mass in the left breast. Mammogram showed many oval masses with circumscribed margins (a–b). These findings were corroborated on ultrasound, exhibiting oval masses with indistinct and microlobulated margins and a heterogeneous echo pattern (c–f). Edema was also evident (e–f). Metastatic melanoma to the breast was confirmed following a histopathological analysis of the breast specimen. HE staining and immunohistochemistry analysis of the metastases. HE staining revealed the malignant cells in the breast tumor (g), and the immunohistochemistry analysis indicated that the cells were positive for HMB45 (h).
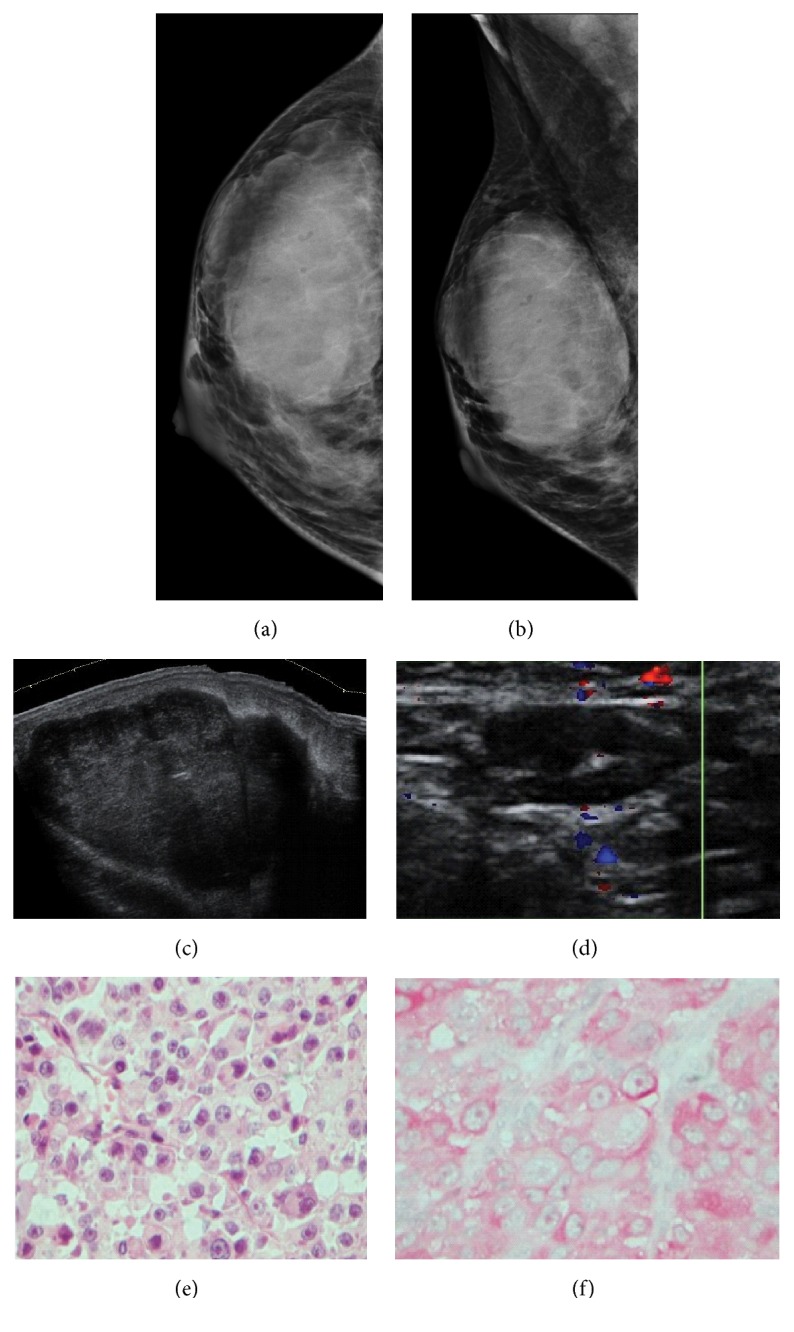
Case
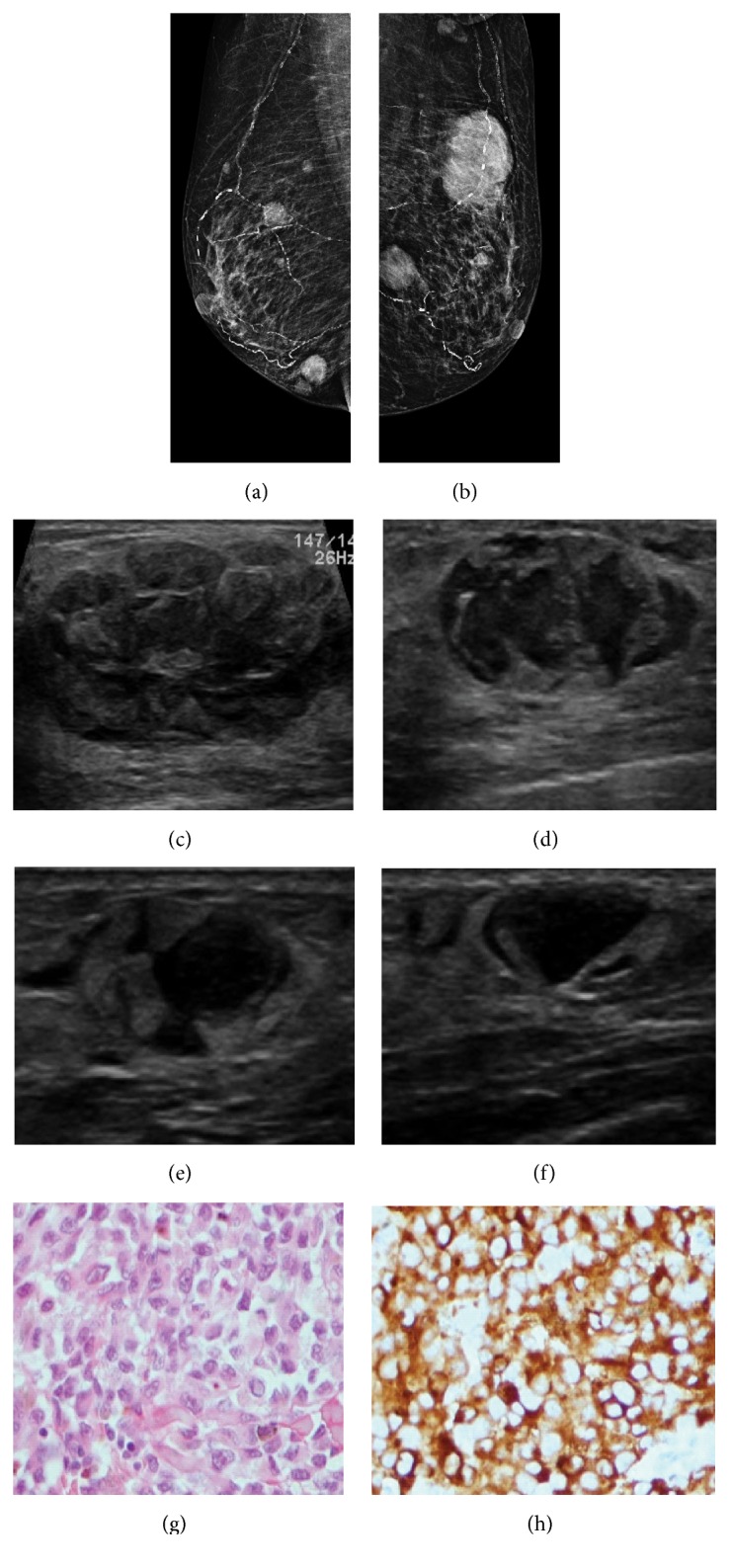
8. A 57-year-old-woman with Epstein–Barr virus (EBV)-associated, extranodal natural killer (NK)-cell lymphoma of nasal type. In 2006, the patient was diagnosed with breast cancer, which was treated with sentinel lymph node (SLN) biopsy and a total mastectomy. In 2016, the patient was admitted to our institution for an unusual nasal blockage and rhinorrhea over a 1-month period. Upon interrogation, the patient also reported progressive loss of vision in the left eye, which was associated with a mass. Notably, a palpable mass was appreciated in the right breast at the time of the evaluation (a). Mammogram showed an irregular mass with indistinct margins occupying the upper-outer quadrant of the right breast (b–e). Grayscale ultrasound demonstrated an irregular, solid mass with indistinct and angular margins, a heterogeneous echo pattern, and posterior features with a combined pattern. HE staining and immunohistochemistry analysis of the metastases. HE staining revealed the malignant cells in the breast tumor (f), and the immunohistochemistry analysis indicated that the cells were positive for CD45 (g), and negative for CKAE1-AE3 (h).
Case
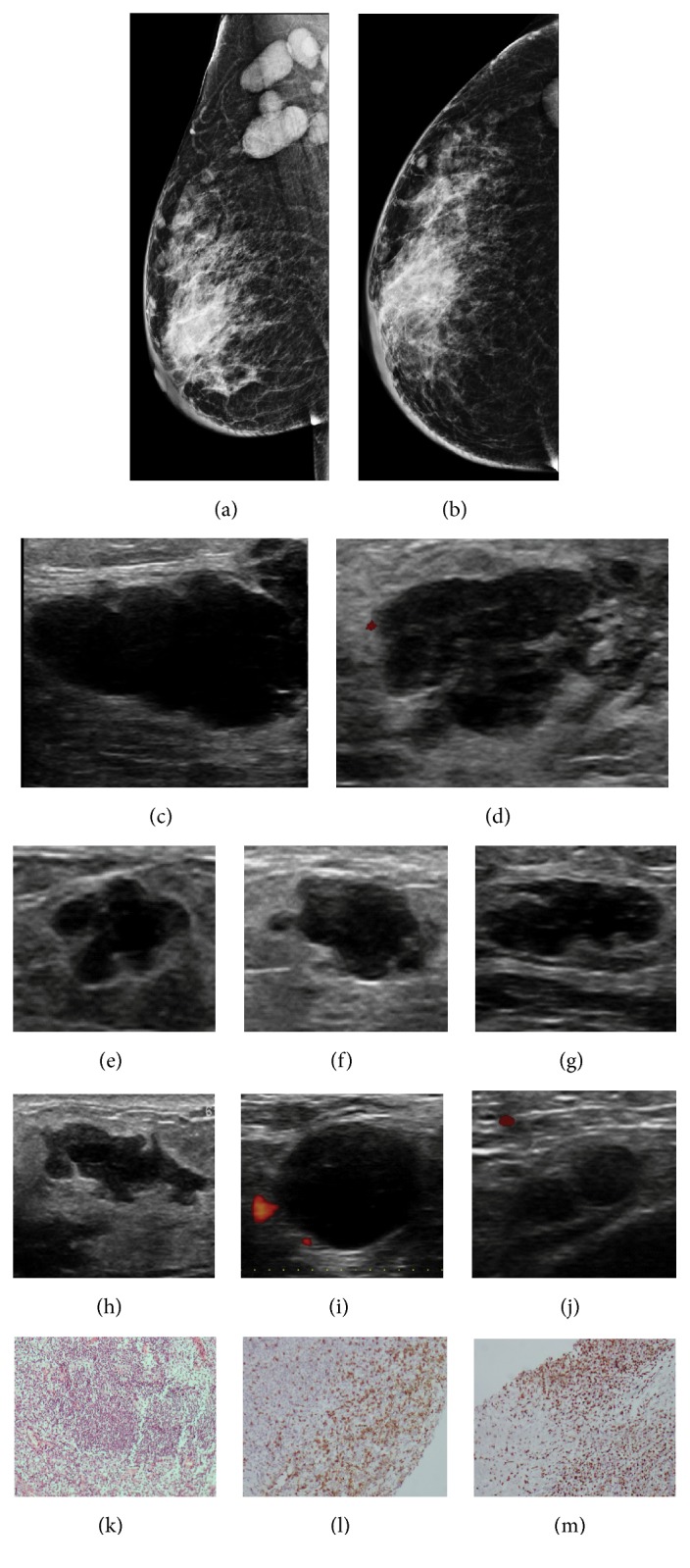
9. A 62-year-old woman with large B-cell lymphoma of germinal center origin. The patient was admitted to our institution for 3 months given the presence of a palpable mass in the right breast (a–b). On mammography, multiple focal asymmetries in the retroareolar region were noted. Additionally, mammograms showed skin thickening and oval masses located on the upper-outer quadrant that were isodense and featured circumscribed margins (c–h). Multiple irregular masses with multilobulated margins and heterogeneous echo patterns were observed on ultrasound (i–j). Both axillary and infraclavicular adenopathies were noticed. HE staining and immunohistochemistry analysis of the metastases. HE staining revealed the malignant cells in the breast tumor (k), and the immunohistochemistry analysis indicated that the cells were positive for CD20 (l). Additionally, it is shown that Ki-67 protein was expressed in 70% of the tumor cells (m).
Case
1
0. A 63-year-old man with gastric signet ring cell carcinoma. One month after diagnosis, the patient presented with a palpable mass in the left breast (b and d). Mammogram showed focal asymmetry in the retroareolar region in the left breast and a high-density mass that resulted in nipple retraction (a–d). On ultrasound, this corresponded to a suspicious, solid heterogeneous mass with indistinct margins and posterior acoustic shadowing (e–f). A comparable lesion was demonstrated in the right breast. HE staining and immunohistochemistry analysis of the metastases. HE staining revealed the malignant cells in the breast tumor (g), and the immunohistochemistry analysis indicated that the cells were positive for PAS (h) and Alcian blue (i).

Case
11. A 40-year-old woman with gastric signet ring-cell carcinoma. A solid mass in the upper-outer quadrant of the right breast was detected on initial exploration. (a–b) Mammogram showed extremely dense parenchyma of the right breast, which corresponded to multiple pseudonodular, hypoechoic, irregular masses with indistinct margins on ultrasound (c–f). HE staining and immunohistochemistry analysis of the metastases. HE staining revealed the malignant cells in the breast tumor (g), and the immunohistochemistry analysis indicated that the cells were positive for MUC5AC (h) and CK20 (j).

Case
1
2. 42-year-old woman with carcinoma of the tongue. One year after diagnosis, the patient presented with a palpable mass in the right breast. On mammography, an irregular, isodense mass was noted in the breast tail (a–b). An oval mass with circumscribed margins and a heterogeneous echo pattern was seen on ultrasound. The lesion also showed posterior acoustic enhancement (c–e), while color Doppler images demonstrated peripheral vascularity (d). HE staining and immunohistochemistry analysis of the metastases. HE staining revealed the malignant cells in the breast tumor (f), and the immunohistochemistry analysis indicated that the cells were positive for P63 (g).
References
-
- Sitzenfrey A. Mammakarzinom zwei jahre nach abdominal radikaloperation wegen doppelseitigen carcinoma ovarii. Prager medizinische Wochenschrift. 1907;32:221–235.
-
- Recine M. A., Deavers M. T., Middleton L. P., Silva E. G., Malpica A. Serous carcinoma of the ovary and peritoneum with metastases to the breast and axillary lymph nodes: a potential pitfall. The American Journal of Surgical Pathology. 2004;28(12):1646–1651. doi: 10.1097/00000478-200412000-00015. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
