

Cost-Effectiveness of Pharmacological Treatments for Osteoporosis Consistent with the Revised Economic Evaluation Guidelines for Canada
- PMID: 30729168
- PMCID: PMC6357295
- DOI: 10.1177/2381468318818843
Cost-Effectiveness of Pharmacological Treatments for Osteoporosis Consistent with the Revised Economic Evaluation Guidelines for Canada
Abstract
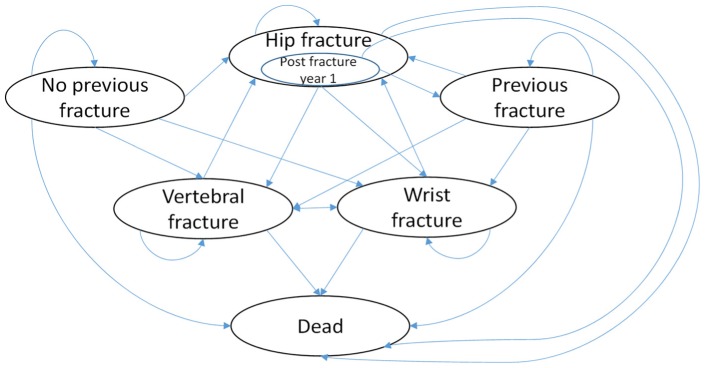
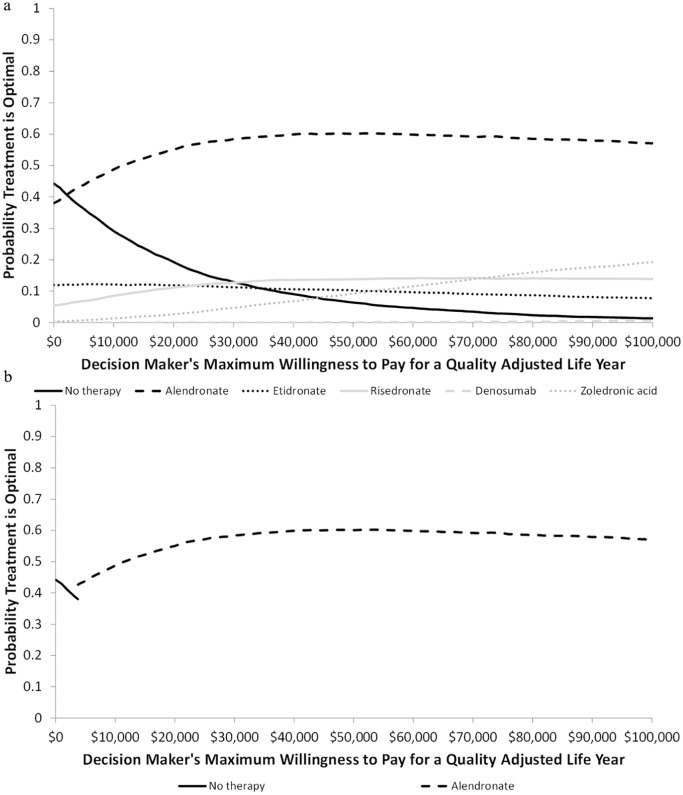
Introduction. Given the lack of independent analyses comparing numerous pharmacotherapies for osteoporosis, the study objective was to identify the optimal osteoporosis treatment based on a woman's age, fracture history, and ability to tolerate oral bisphosphonates adopting practices recommended in the recently revised Canadian guidelines. Methods. A cost utility analysis from the health care system perspective compared alendronate, etidronate, risedronate, zoledronate, denosumab, and no pharmacotherapy using a Markov model incorporating data on fracture risk and their associated costs, mortality, and disutility and treatment effect. Stratified analysis was conducted based on age, fracture history, and ability to tolerate oral bisphosphonates. Expected lifetime outcomes were obtained through probabilistic analysis with scenario analyses addressing methodological and structural uncertainty. Results. For women able to tolerate oral bisphosphonates, risedronate and etidronate were dominated. Compared to no therapy, alendronate was either dominant or was associated with a low incremental cost per QALY (quality-adjusted life years) gained (ICER)-less than CAN$3,751 based on age and fracture history. In comparison with alendronate, both zoledronate and denosumab were either dominated or associated with a high ICER-greater than CAN$660,000 per QALY. For women unable to tolerate bisphosphonates, dependent on age and fracture history, the ICER for zoledronate versus no therapy ranged from CAN$17,770 to CAN$94,365 per QALY. For all strata, denosumab was dominated by zoledronate or had an ICER greater than CAN$3.0 million. Scenario analyses found consistent findings. Conclusions. Based on a threshold of CAN$50,000 per QALY, alendronate is optimal for osteoporotic women who can tolerate oral bisphosphonates regardless of age or fracture history. For women unable to tolerate oral bisphosphonates, zoledronate is optimal for women with previous fracture or aged 80 to 84 or over 90 with no previous fracture.
Keywords: bisphosphonates; cost-effectiveness; osteoporosis.
Figures
Similar articles
-
Cost effectiveness of denosumab versus oral bisphosphonates for postmenopausal osteoporosis in the US.Appl Health Econ Health Policy. 2013 Oct;11(5):485-97. doi: 10.1007/s40258-013-0047-8. Appl Health Econ Health Policy. 2013. PMID: 23868102
-
Denosumab: a cost-effective alternative for older men with osteoporosis from a Swedish payer perspective.Bone. 2014 Feb;59:105-13. doi: 10.1016/j.bone.2013.11.002. Epub 2013 Nov 12. Bone. 2014. PMID: 24231131
-
Health-economic comparison of three recommended drugs for the treatment of osteoporosis.Int J Clin Pharmacol Res. 2004;24(1):1-10. Int J Clin Pharmacol Res. 2004. PMID: 15575171
-
Denosumab: A Unique Perspective on Adherence and Cost-effectiveness Compared With Oral Bisphosphonates in Osteoporosis Patients.Ann Pharmacother. 2018 Oct;52(10):1031-1041. doi: 10.1177/1060028018768808. Epub 2018 Apr 4. Ann Pharmacother. 2018. PMID: 29616561 Review.
-
Bisphosphonate treatment of osteoporosis.Clin Geriatr Med. 2003 May;19(2):395-414. doi: 10.1016/s0749-0690(02)00069-1. Clin Geriatr Med. 2003. PMID: 12916293 Review.
Cited by
-
An Updated Systematic Review of Cost-Effectiveness Analyses of Drugs for Osteoporosis.Pharmacoeconomics. 2021 Feb;39(2):181-209. doi: 10.1007/s40273-020-00965-9. Epub 2020 Oct 7. Pharmacoeconomics. 2021. PMID: 33026634 Free PMC article.
-
Awareness of osteoporosis risk assessment tools and screening recommendations among community pharmacists in Malaysia.Int J Clin Pharm. 2021 Jun;43(3):604-612. doi: 10.1007/s11096-020-01169-z. Epub 2021 Jan 28. Int J Clin Pharm. 2021. PMID: 33507463
-
Actualisation 2023 des lignes directrices de pratique clinique pour la prise en charge de l’ostéoporose et la prévention des fractures au Canada.CMAJ. 2023 Nov 26;195(46):E1585-E1603. doi: 10.1503/cmaj.221647-f. CMAJ. 2023. PMID: 38011931 Free PMC article. French.
-
Cost-effectiveness of integrated disease management for high risk, exacerbation prone, patients with chronic obstructive pulmonary disease in a primary care setting.Cost Eff Resour Alloc. 2022 Aug 12;20(1):39. doi: 10.1186/s12962-022-00377-w. Cost Eff Resour Alloc. 2022. PMID: 35962399 Free PMC article.
-
Clinical practice guideline for management of osteoporosis and fracture prevention in Canada: 2023 update.CMAJ. 2023 Oct 10;195(39):E1333-E1348. doi: 10.1503/cmaj.221647. CMAJ. 2023. PMID: 37816527 Free PMC article.
References
-
- World Health Organization. The Assessment of Osteoporosis at Primary Health Care Level. Geneva: World Health Organization; 2007.
-
- Qaseem A, Forciea MA, Mclean RM, Denberg TD; Clinical Guidelines Committee of the American College of Physicians. Treatment of low bone density or osteoporosis to prevent fractures in men and women: a clinical practice guideline update from the American College of Physicians. Ann Intern Med. 2017;166(11):818–39. doi:10.7326/M15-1361 - DOI - PubMed
-
- Tenenhouse A, Joseph L, Kreiger N, et al. Estimation of the prevalence of low bone density in Canadian women and men using a population-specific DXA reference standard: the Canadian Multicentre Osteoporosis Study (CaMos). Osteoporos Int. 2000;11(10):897–904. - PubMed
LinkOut - more resources
Full Text Sources
