

Thulium fiber laser: the new player for kidney stone treatment? A comparison with Holmium:YAG laser
- PMID: 30729311
- PMCID: PMC7363731
- DOI: 10.1007/s00345-019-02654-5
Thulium fiber laser: the new player for kidney stone treatment? A comparison with Holmium:YAG laser
Abstract
Purpose: To compare the operating modes of the Holmium:YAG laser and Thulium fiber laser. Additionally, currently available literature on Thulium fiber laser lithotripsy is reviewed.
Materials and methods: Medline, Scopus, Embase, and Web of Science databases were searched for articles relating to the operating modes of Holmium:YAG and Thulium fiber lasers, including systematic review of articles on Thulium fiber laser lithotripsy.
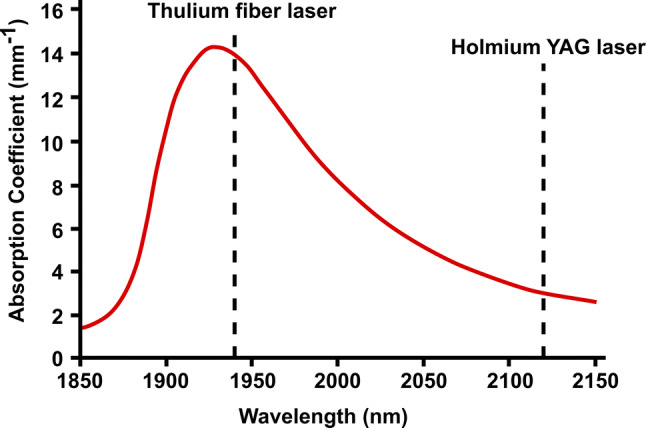
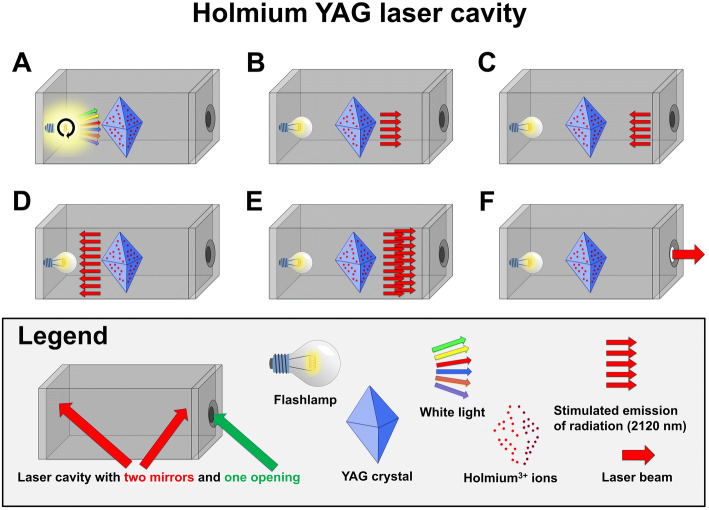
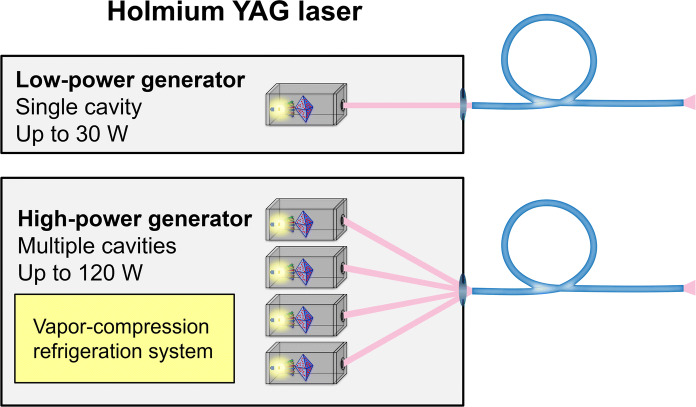
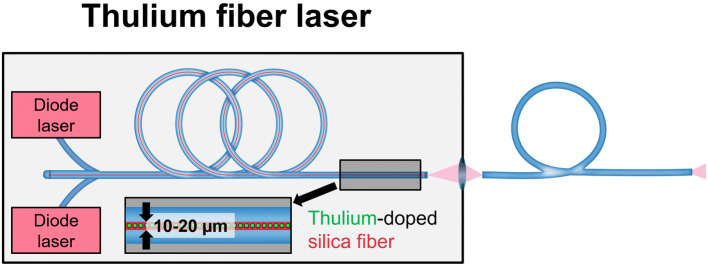
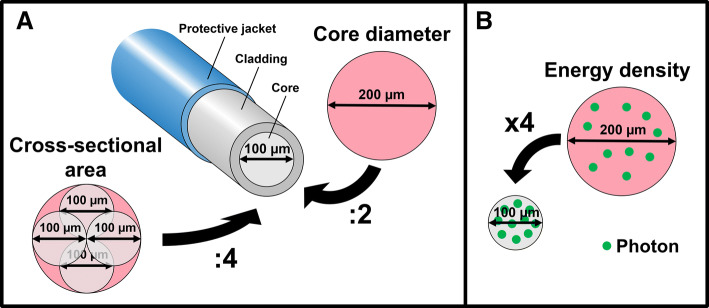
Results: The laser beam emerging from the Holmium:YAG laser involves fundamental architectural design constraints compared to the Thulium fiber laser. These differences translate into multiple potential advantages in favor of the Thulium fiber laser: four-fold higher absorption coefficient in water, smaller operating laser fibers (50-150 µm core diameter), lower energy per pulse (as low as 0.025 J), and higher maximal pulse repetition rate (up to 2000 Hz). Multiple comparative in vitro studies suggest a 1.5-4 times faster stone ablation rate in favor of the Thulium fiber laser.
Conclusions: The Thulium fiber laser overcomes the main limitations reported with the Holmium:YAG laser relating to lithotripsy, based on preliminary in vitro studies. This innovative laser technology seems particularly advantageous for ureteroscopy and may become an important milestone for kidney stone treatment.
Keywords: Holmium:YAG laser; Innovation; Lithotripsy; Thulium fiber laser; Urinary stone.
Conflict of interest statement
Prof. Olivier Traxer is a consultant for Coloplast, Rocamed, Olympus, EMS, Boston Scientific and IPG Medical.
Figures
Comment in
-
Laser absorption coefficient of thulium fiber laser and holmium Yag laser: in what scale.World J Urol. 2023 Apr;41(4):1207-1208. doi: 10.1007/s00345-023-04331-0. Epub 2023 Mar 6. World J Urol. 2023. PMID: 36877267 No abstract available.
References
-
- Sayer J, Johnson DE, Price RE, Cromeens DM. Ureteral lithotripsy with the Holmium:YAG laser. J Clin Laser Med Surg. 1993;11(2):61–65. doi: 10.1089/clm.1993.11.61. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
