

Risk factors for nonunion after intramedullary nailing of subtrochanteric femoral fractures
- PMID: 30729990
- PMCID: PMC6514068
- DOI: 10.1007/s00402-019-03131-9
Risk factors for nonunion after intramedullary nailing of subtrochanteric femoral fractures
Abstract
Introduction: Nonunion is a common complication after intramedullary nailing of subtrochanteric femoral fractures. A more detailed knowledge, particularly of avoidable risk factors for subtrochanteric fracture nonunion, is thus desired to develop strategies for reducing nonunion rates. The aim of the present study therefore was to analyse a wide range of parameters as potential risk factors for nonunion after intramedullary nailing of subtrochanteric fractures.
Materials and methods: Seventy-four patients who sustained a subtrochanteric fracture and were treated by femoral intramedullary nailing at a single level 1 trauma centre within a 6-year period were included in this study. A total of 15 patient-related, fracture-related, surgery-related, mechanical and biological parameters were analysed as potential risk factors for nonunion. Furthermore, the accuracy of each of these parameters to predict nonunion was calculated.
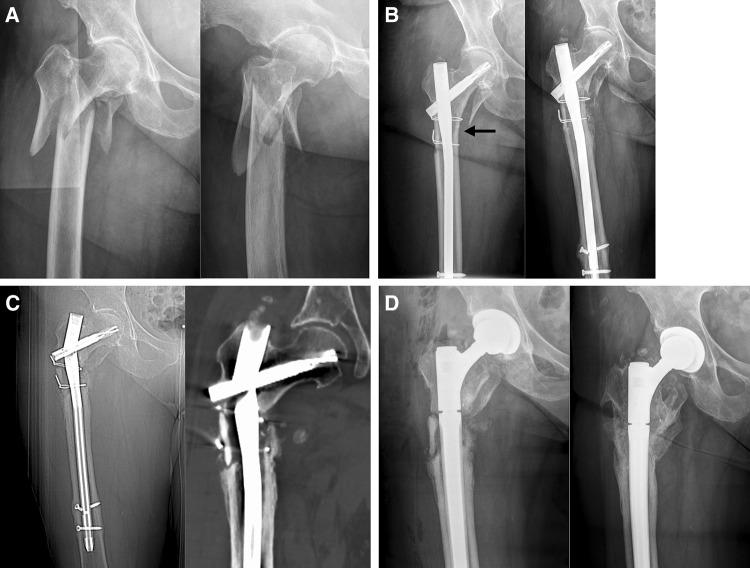
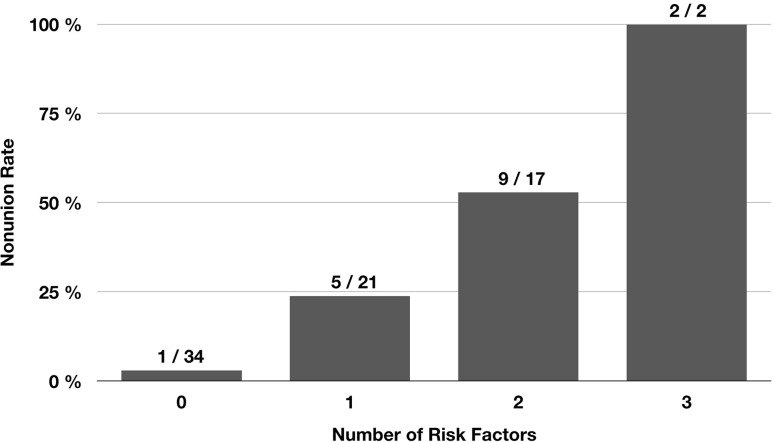
Results: Nonunion occurred in 17 of 74 patients (23.0%). Of the 15 potential risk factors analysed, only 3 were found to have a significant effect on the nonunion rate (p < 0.05): postoperative varus malalignment, postoperative lack of medial cortical support and autodynamisation of the nail within the first 12 weeks post-surgery. Accuracy of each of these 3 parameters to predict nonunion was > 0.70. Furthermore, the nonunion rate significantly increased with the number of risk factors (no risk factor: 2.9%, one risk factor: 23.8%, two risk factors: 52.9%, and three risk factors: 100% [Chi-square test, p = 0.001)].
Conclusions: Our study indicates that intraoperative correction of varus malalignment and restoration of the medial cortical support are the most critical factors to prevent nonunion after intramedullary nailing of subtrochanteric femoral fractures. In addition, autodynamisation of the nail within the first 3 months post-surgery is a strong predictor for failure and should result in revision surgery.
Keywords: Femoral fracture; Femoral nailing; Intramedullary nailing; Nonunion; Pseudarthrosis; Risk factors; Subtrochanteric femoral fracture; Subtrochanteric fracture.
Conflict of interest statement
All authors declare that they have no conflict of interest. No funding was received for the study.
Figures


References
-
- Codesido P, Mejía A, Riego J, Ojeda-Thies C. Subtrochanteric fractures in elderly people treated with intramedullary fixation: quality of life and complications following open reduction and cerclage wiring versus closed reduction. Arch Orthop Trauma Surg. 2017;137:1077–1085. doi: 10.1007/s00402-017-2722-y. - DOI - PubMed
-
- Bogdan Y, Tornetta P, Einhorn TA, Guy P, Leveille L, Robinson J, et al. Healing time and complications in operatively treated atypical femur fractures associated with bisphosphonate use: a multicenter retrospective cohort. J Orthop Trauma. 2016;30:177–181. doi: 10.1097/BOT.0000000000000516. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
