

Computed tomography scan contribution to the diagnosis of community-acquired pneumonia
- PMID: 30730311
- PMCID: PMC6455090
- DOI: 10.1097/MCP.0000000000000567
Computed tomography scan contribution to the diagnosis of community-acquired pneumonia
Abstract
Purpose of review: Pneumonia is a frequent disease mainly affecting older and multimorbid patients. Symptoms and signs lack sensitivity and specificity, and chest X-ray has poor accuracy. Hence, an initial diagnosis of pneumonia has limited predictive value for the presence of pneumonia. Overdiagnosis of pneumonia leads to inappropriate antibiotic use and may delay the appropriate management of mimicking diseases. Alternative imaging strategies including computed tomography (CT)-scan or lung ultrasonography may improve the diagnosis of pneumonia. We review the recent evidence and perspectives regarding their contribution to the diagnosis and management of patients with suspected pneumonia.
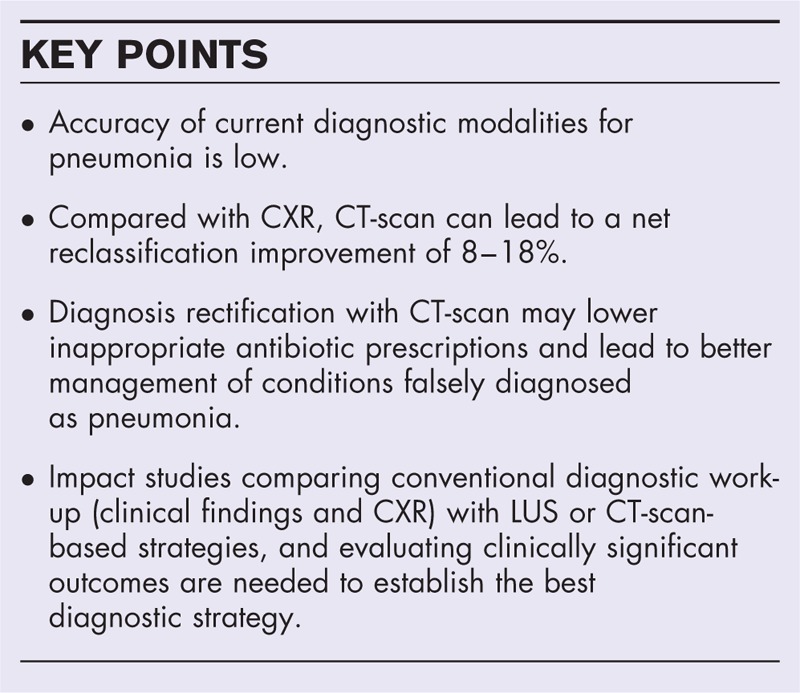
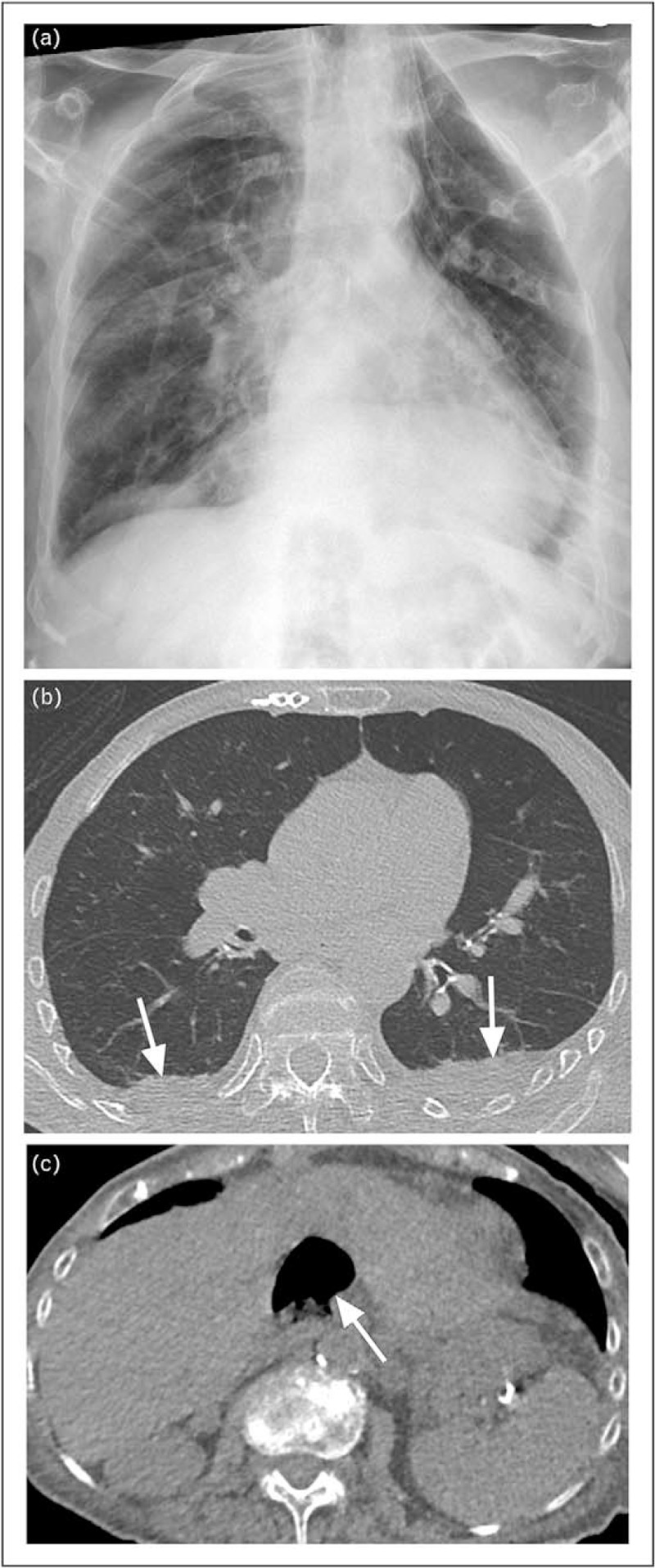
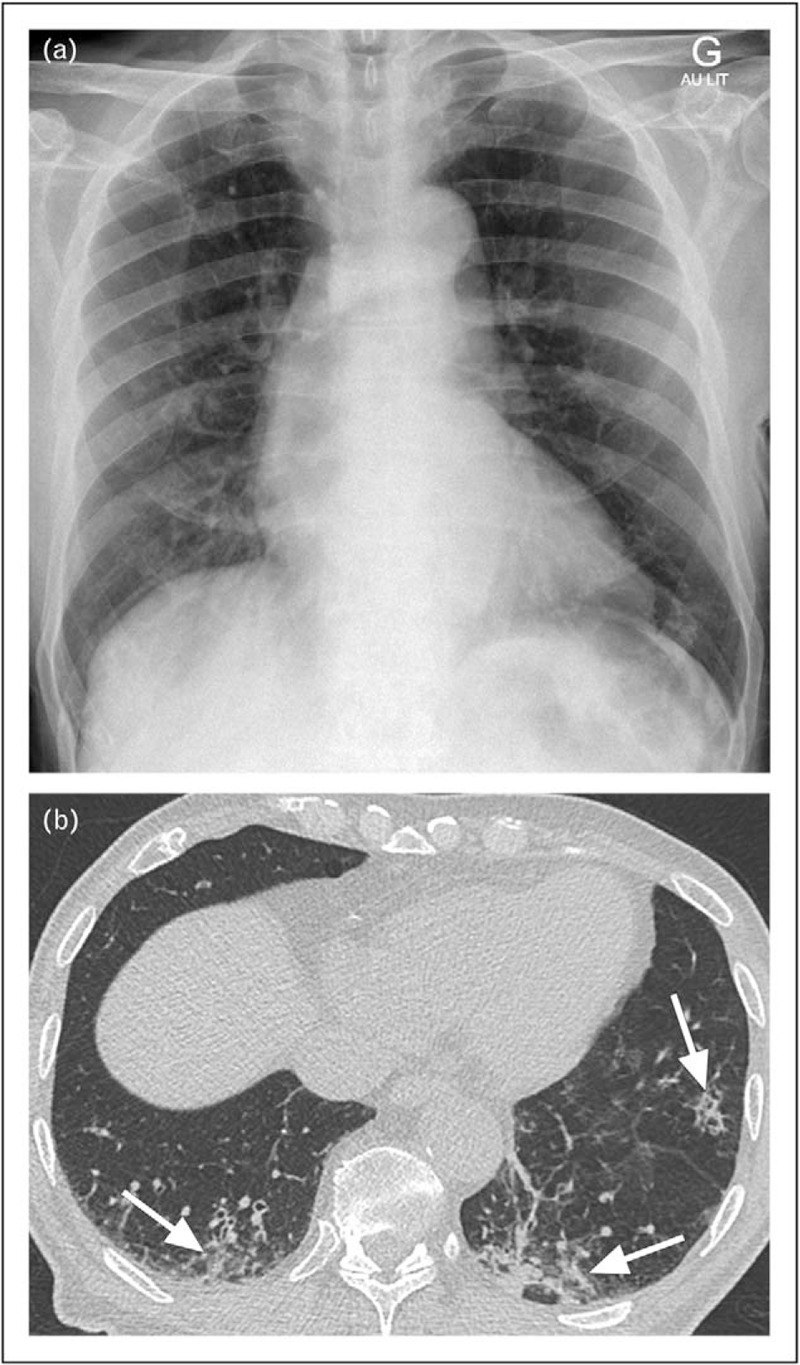
Recent findings: Two studies assessed the diagnostic accuracy of CT-scan in emergency department or hospitalized patients suspected of pneumonia. CT-scan led to a net reclassification improvement of 8 and 18% of patients, and was particularly helpful to rule out the diagnosis, allowing a lowering of the number of inappropriate antibiotic prescriptions.
Summary: CT-scan reduces overdiagnosis of pneumonia and allows a better identification of alternative diagnoses. The impact on clinical outcomes of a strategy incorporating CT-scan for patients suspected of pneumonia should be evaluated, along with its cost-effectiveness.
Figures
References
-
- Shapiro DJ, Hicks LA, Pavia AT, Hersh AL. Antibiotic prescribing for adults in ambulatory care in the USA, 2007-09. J Antimicrob Chemother 2014; 69:234–240. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
