

Comparison of Micro-Computed Tomography and Clinical Computed Tomography Protocols for Visualization of Nasal Cartilage Before Surgical Planning for Rhinoplasty
- PMID: 30730533
- PMCID: PMC6537836
- DOI: 10.1001/jamafacial.2018.1931
Comparison of Micro-Computed Tomography and Clinical Computed Tomography Protocols for Visualization of Nasal Cartilage Before Surgical Planning for Rhinoplasty
Abstract
Importance: There is no imaging standard to model nasal cartilage for the planning of rhinoplasty procedures. Preoperative visualization of cartilage may improve objective evaluation of nasal deformities, surgical planning, and surgical reconstruction.
Objectives: To evaluate the feasibility of visualizing nasal cartilage using high resolution micro-computed tomography (CT) compared with the criterion standard of pathologic findings in a cadaveric specimen and to evaluate its accuracy compared with various clinical CT protocols.
Design, setting, and participants: Anatomic study at the University of Washington using single human cadaveric nasal specimens performed from July 10, 2017, to March 30, 2018.
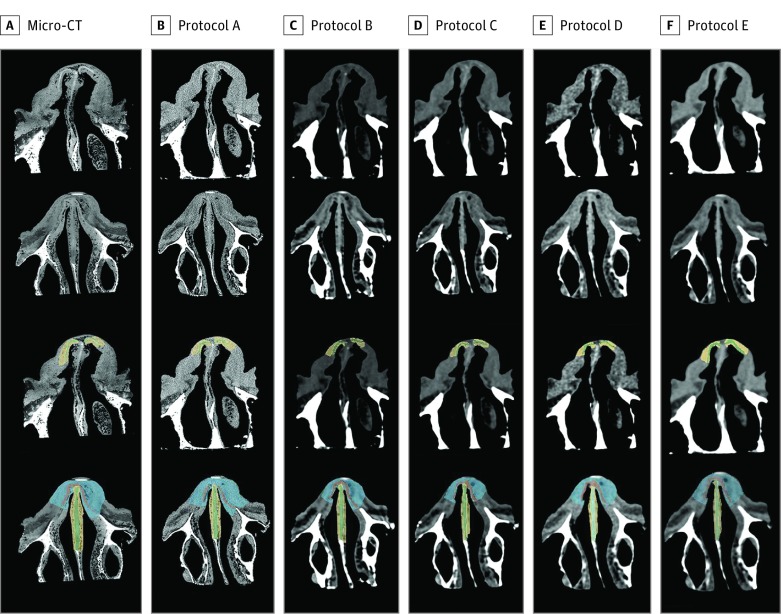
Interventions: A micro-CT acquisition with 60-micron resolution was obtained of a nasal specimen. The specimen was then scanned with 5 different clinical CT protocols to span both clinical care and machine limits. The specimen was then sectioned in 5-mm axial slices for pathologic analysis.
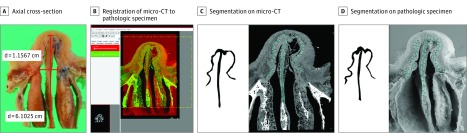
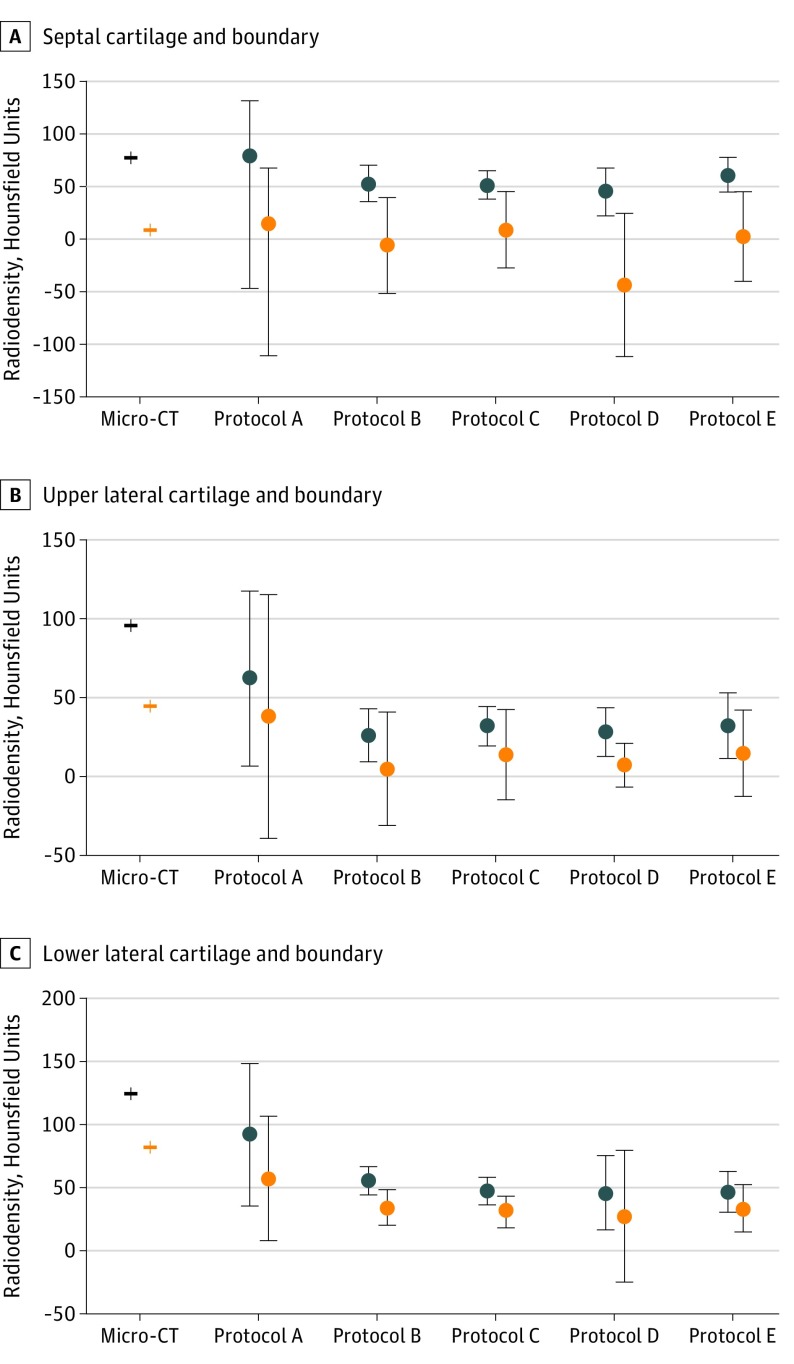
Main outcomes and measures: Micro-CT images were registered to pathologic specimen cross-sections using a graphite fiducial system. Cartilage substructures were manually segmented and analyzed. A library of matched images across the micro-CT and various clinical CT protocols was then developed. Region of interest analysis was performed for each of the cartilage structures and their boundaries on clinical CT protocols and micro-CT, with the outcome of mean (SD) density using Hounsfield units.
Results: A single human cadaveric nasal specimen was used to obtain the following results. Lower lateral cartilage, upper lateral cartilage, and septal cartilage were accurately delineated on the micro-CT images compared with pathologic findings. The mean absolute deviation from pathologic findings was 0.30 mm for septal cartilage thickness, 0.98 mm for maximal upper lateral cartilage length, and 1.40 mm for maximal lower lateral cartilage length. On clinical CT protocols, only septal cartilage was well discriminated from boundary. Higher radiation dose resulted in more accurate density measurements of cartilage, but it did not ultimately improve ability to discriminate cartilage.
Conclusions and relevance: The results of this anatomic study may represent a notable step toward advancing knowledge of the capabilities and pitfalls of nasal cartilage visualization on CT. Nasal cartilage visualization was feasible on the micro-CT compared with pathologic findings. Future research may further examine the barriers to accurately visualizing upper lateral cartilage and lower lateral cartilage, a prerequisite for clinical application.
Level of evidence: NA.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials