

Late Morbidity and Mortality Among Medulloblastoma Survivors Diagnosed Across Three Decades: A Report From the Childhood Cancer Survivor Study
- PMID: 30730781
- PMCID: PMC6424138
- DOI: 10.1200/JCO.18.00969
Late Morbidity and Mortality Among Medulloblastoma Survivors Diagnosed Across Three Decades: A Report From the Childhood Cancer Survivor Study
Abstract
Purpose: Treatment of medulloblastoma has evolved from surgery and radiotherapy to contemporary multimodal regimens. However, the impact on long-term health outcomes remains unknown.
Methods: Cumulative incidence of late mortality (5 or more years from diagnosis), subsequent neoplasms (SNs), and chronic health conditions were evaluated in the Childhood Cancer Survivor Study among 5-year survivors of medulloblastoma diagnosed between 1970 and 1999. Outcomes were evaluated by treatment exposure, including historical therapy (craniospinal irradiation [CSI] ≥ 30 Gy, no chemotherapy), high risk (CSI ≥ 30 Gy + chemotherapy), standard risk (CSI < 30 Gy + chemotherapy), and by treatment decade (1970s, 1980s, 1990s). Rate ratios (RRs) and 95% CIs estimated long-term outcomes using multivariable piecewise exponential models.
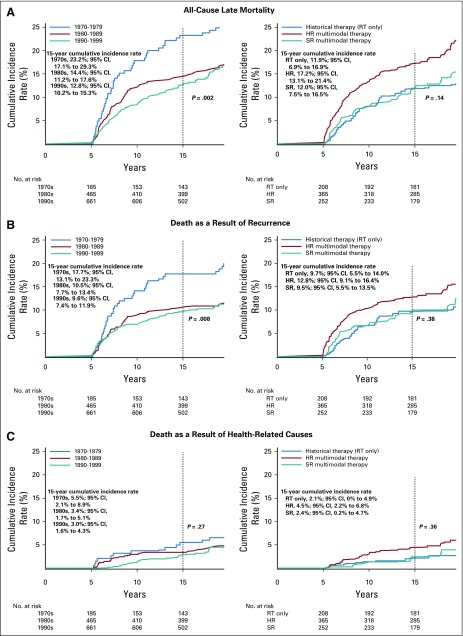
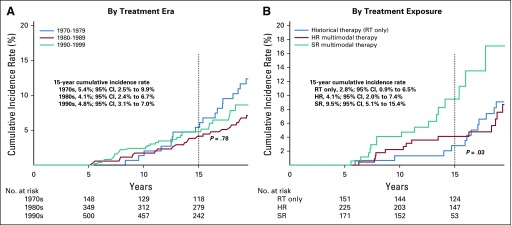
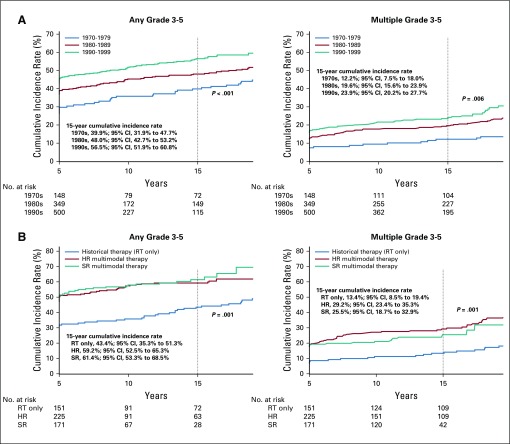
Results: Among 1,311 eligible survivors (median age, 29 years [range, 6 to 60 years]; median time from diagnosis, 21 years [range, 5 to 44 years]), the 15-year cumulative incidence rate of all-cause late mortality was 23.2% (diagnosed 1970s) versus 12.8% (1990s; P = .002), with a recurrence-related mortality rate of 17.7% versus 9.6% ( P = .008). Lower late mortality rates as a result of other health-related causes were not observed. Among 997 survivors who completed a baseline survey, the 15-year cumulative incidence of SNs was higher among survivors with multimodal therapy (standard risk, 9.5%; historical, 2.8%; P = .03). Survivors treated in the 1990s had a higher cumulative incidence of severe, disabling, life-threatening, and fatal chronic health conditions (56.5% in 1990s v 39.9% in 1970s; P < .001) and were more likely to develop multiple conditions (RR, 2.89; 95% CI, 1.31 to 6.38). However, survivors of standard-risk therapy were less likely to use special education services than high-risk therapy survivors (RR, 0.84; 95% CI, 0.75 to 0.93).
Conclusion: Historical changes in medulloblastoma therapy that improved 5-year survival have increased the risk for SNs and debilitating health conditions for survivors yet reduced the need for special education services.
Figures
References
-
- Massimino M, Biassoni V, Gandola L, et al. Childhood medulloblastoma. Crit Rev Oncol Hematol. 2016;105:35–51. - PubMed
-
- Packer RJ, Gajjar A, Vezina G, et al. Phase III study of craniospinal radiation therapy followed by adjuvant chemotherapy for newly diagnosed average-risk medulloblastoma. J Clin Oncol. 2006;24:4202–4208. - PubMed
-
- Gajjar A, Chintagumpala M, Ashley D, et al. Risk-adapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in children with newly diagnosed medulloblastoma (St Jude Medulloblastoma-96): Long-term results from a prospective, multicentre trial. Lancet Oncol. 2006;7:813–820. - PubMed
-
- von Bueren AO, Kortmann RD, von Hoff K, et al. Treatment of children and adolescents with metastatic medulloblastoma and prognostic relevance of clinical and biologic parameters. J Clin Oncol. 2016;34:4151–4160. - PubMed
-
- Paterson E, Farr RF. Cerebellar medulloblastoma: Treatment by irradiation of the whole central nervous system. Acta Radiol. 1953;39:323–336. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
