

Heart failure and adverse heart failure outcomes among persons living with HIV in a US tertiary medical center
- PMID: 30731372
- PMCID: PMC6441629
- DOI: 10.1016/j.ahj.2019.01.002
Heart failure and adverse heart failure outcomes among persons living with HIV in a US tertiary medical center
Abstract
Background: Persons living with HIV (PLHIV) have an increased risk of heart failure (HF). However, little is known about outcomes among PLHIV with HF. The study aim was to compare HF outcomes among PLHIV with HF versus individuals without HIV with HF.
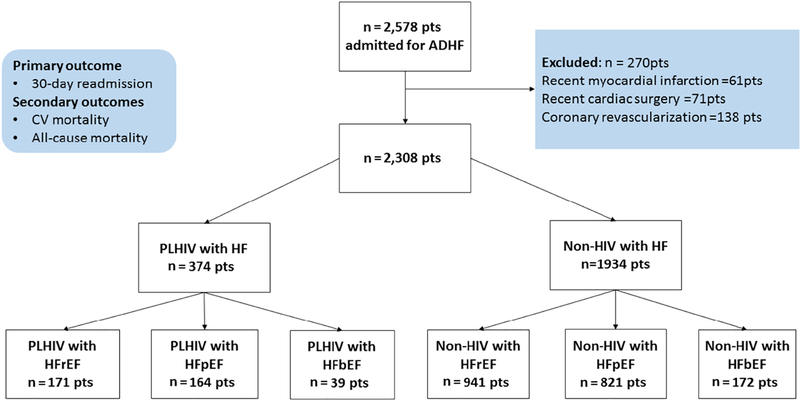
Methods: Our cohort included 2,308 individuals admitted with decompensated HF. We compared baseline characteristics, 30-day HF readmission, and cardiovascular (CV) and all-cause mortality. Within PLHIV, we assessed outcomes stratified between CD4 count and viral load (VL), and tested the association between traditional and HIV-specific parameters with 30-day HF readmission.
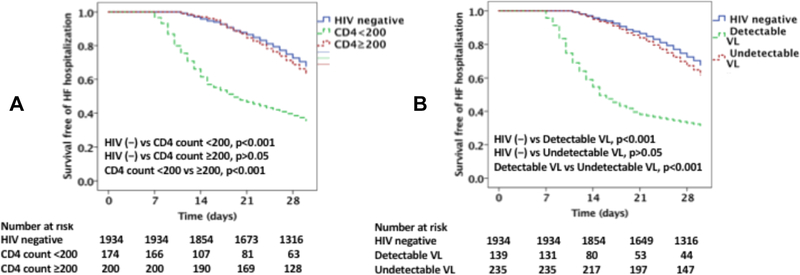
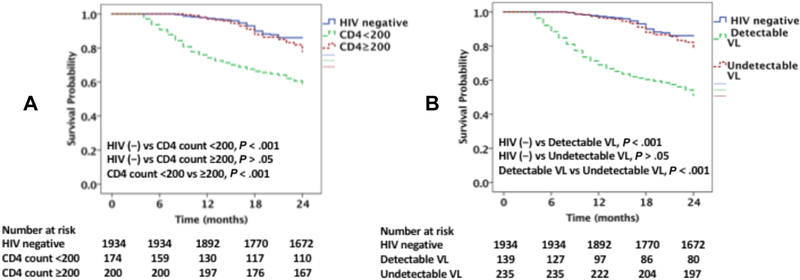
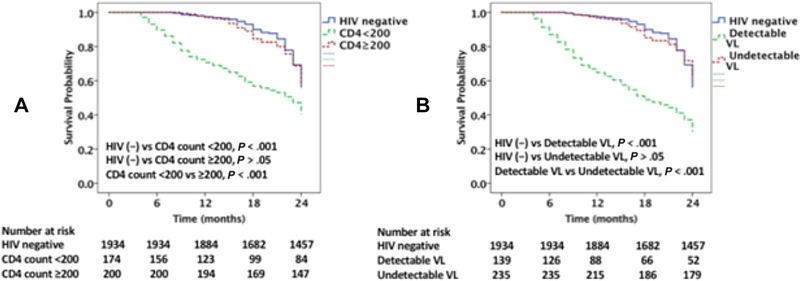
Results: There were 374 (16%) PLHIV with HF. Among PLHIV, 92% were on antiretroviral therapy and 63% had a VL <200 copies/mL. Groups were similar with respect to age, sex, race/ethnicity, and CV risk factors. In follow-up, PLHIV had increased 30-day HF readmission (49% vs 32%) and CV (26% vs 13.5%) and all-cause mortality rates (38% vs 22%). Among PLHIV, cocaine use, HIV-specific parameters (CD4, VL), and coronary artery disease were predictors of 30-day HF readmission. Specifically, among PLHIV, those with detectable VL had higher 30-day HF readmission and CV mortality, whereas PLHIV with undetectable VL had a similar 30-day HF readmission rate and CV mortality to uninfected controls with HF. Similar outcomes were observed across strata of left ventricular ejection fraction and by CD4.
Conclusions: PLHIV with a low CD4 count or detectable VL have an increased 30-day HF readmission rate as well as increased CV and all-cause mortality. In contrast, PLHIV with a higher CD4 count and undetectable VL have similar HF outcomes to uninfected controls.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest statement
The authors do not have any commercial or other association that might pose a conflict of interest.
Figures
References
-
- Lohse N, Obel N. Update of Survival for Persons With HIV Infection in Denmark. Ann Intern Med 2016;165(10):749–750. - PubMed
-
- Samji H, Cescon A, Hogg RS, Modur SP, Althoff KN, Buchacz K, Burchell AN, Cohen M, Gebo KA, Gill MJ, Justice A, Kirk G, Klein MB, Korthuis PT, Martin J, Napravnik S, Rourke SB, Sterling TR, Silverberg MJ, Deeks S, Jacobson LP, Bosch RJ, Kitahata MM, Goedert JJ, Moore R, Gange SJ, North American ACCoR, Design of Ie DEA. Closing the gap: increases in life expectancy among treated HIV-positive individuals in the United States and Canada. PLoS One 2013;8(12):e81355. - PMC - PubMed
-
- WHO HIV Statsitics: http://www.who.int/hiv/data/en/. In; 2016.
-
- Freiberg MS, Chang CH, Skanderson M, Patterson OV, DuVall SL, Brandt CA, So-Armah KA, Vasan RS, Oursler KA, Gottdiener J, Gottlieb S, Leaf D, Rodriguez-Barradas M, Tracy RP, Gibert CL, Rimland D, Bedimo RJ, Brown ST, Goetz MB, Warner A, Crothers K, Tindle HA, Alcorn C, Bachmann JM, Justice AC, Butt AA. Association Between HIV Infection and the Risk of Heart Failure With Reduced Ejection Fraction and Preserved Ejection Fraction in the Antiretroviral Therapy Era: Results From the Veterans Aging Cohort Study. JAMA Cardiol 2017;2(5):536–546. - PMC - PubMed
-
- Butt AA, Chang CC, Kuller L, Goetz MB, Leaf D, Rimland D, Gibert CL, Oursler KK, Rodriguez-Barradas MC, Lim J, Kazis LE, Gottlieb S, Justice AC, Freiberg MS. Risk of heart failure with human immunodeficiency virus in the absence of prior diagnosis of coronary heart disease. Arch Intern Med 2011;171(8):737–43. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
