

Imaging findings of intraductal tubulopapillary neoplasm (ITPN) of the pancreas: Two case reports and literature review
- PMID: 30732200
- PMCID: PMC6380796
- DOI: 10.1097/MD.0000000000014426
Imaging findings of intraductal tubulopapillary neoplasm (ITPN) of the pancreas: Two case reports and literature review
Abstract
Rationale: Intraductal tubulopapillary neoplasm (ITPN) is a rare type of pancreatic epithelial neoplasm. We report 2 cases of ITPN and detail the imaging findings.
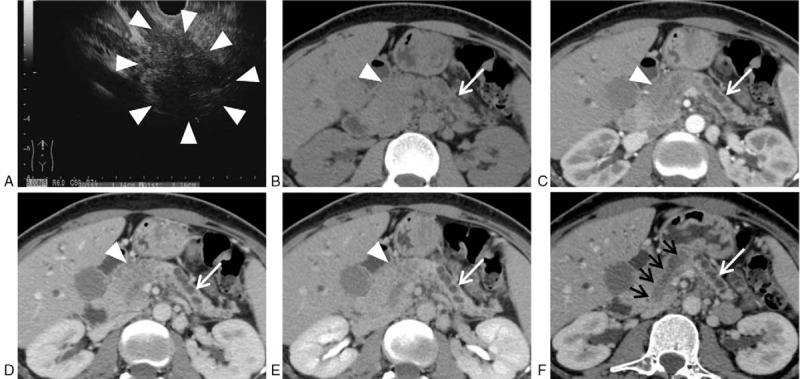
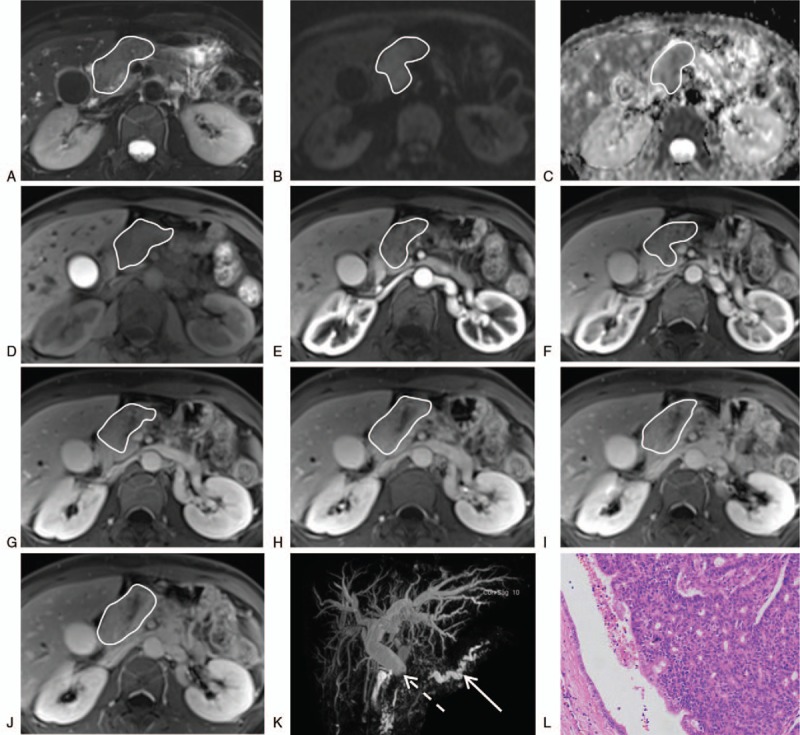
Patient concerns: The 1st case was a 36-year-old woman who complained of jaundice, yellow urine and diarrhea. She accepted ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI) examination before surgery, which all revealed a mass in the pancreatic head. The 2nd case was a 62-year-old woman who was admitted to our hospital for the treatment of a pancreatic tumor. The MRI showed a mass filled the mian pancreatic duct in the head and neck.
Diagnosis: The ITPN is an intraductal, grossly visible, tubule-forming epithelial neoplasm with high-grade dysplasia and ductal differentiation without overt mucin production.
Interventions: The 1st patient received percutaneous transhepatic cholangial drainage procedure, endoscopic ultrasound guided fine needle aspiration, pancreatoduodenectomy, cholecystectomy, and lymphadenectomy successively. The 2nd patient received pancreaticoduodenectomy, cholecystectomy, and partial gastrectomy.
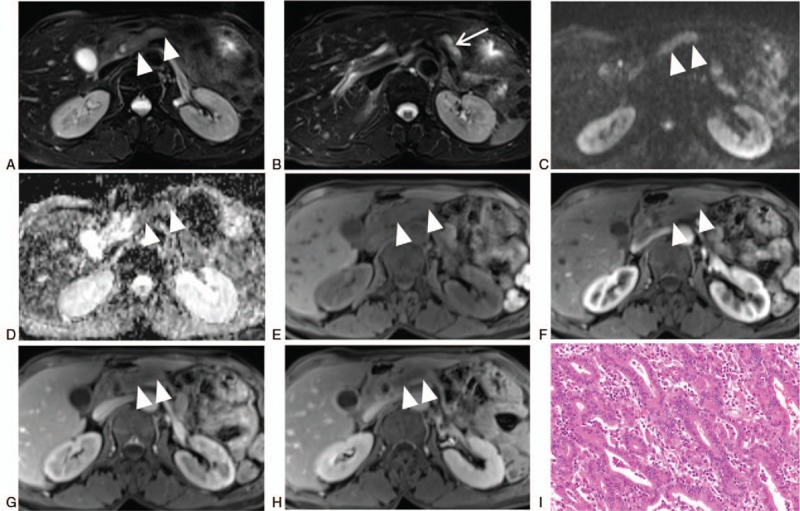
Outcomes: Two months after surgery, the follow-up MRI revealed hepatic metastasis of the 1st patient. She is still alive now. The 2nd patient was lost to follow-up.
Lessons: The ITPN is a rare pancreatic neoplasm and its clinical symptoms are atypical. It is difficult to make accurate diagnosis of ITPN before surgery even though various imaging modalities are used in combination. When a solid mass growing in the lumen of the pancreatic duct, ITPN should be taken into consideration.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
A case of intraductal tubulopapillary neoplasm of the pancreas in a branch duct: a rare case report and literature review.BMC Gastroenterol. 2021 Apr 13;21(1):162. doi: 10.1186/s12876-021-01744-2. BMC Gastroenterol. 2021. PMID: 33849435 Free PMC article. Review.
-
Intraductal tubulopapillary neoplasm of the pancreas on fine needle aspiration: case report with differential diagnosis.Diagn Cytopathol. 2014 Feb;42(2):156-60. doi: 10.1002/dc.22890. Epub 2012 Jul 16. Diagn Cytopathol. 2014. PMID: 22807417
-
Intraductal tubulopapillary neoplasm (ITPN) of the pancreas associated with an invasive component: a case report with review of the literature.World J Surg Oncol. 2017 Nov 16;15(1):203. doi: 10.1186/s12957-017-1267-4. World J Surg Oncol. 2017. PMID: 29145864 Free PMC article. Review.
-
[A rare case of intraductal tumor of the pancreas in which an intraductal tubulopapillary neoplasm was mixed with a widely spreading gastric-type intraductal papillary-mucinous neoplasm].Nihon Shokakibyo Gakkai Zasshi. 2024;121(5):415-424. doi: 10.11405/nisshoshi.121.415. Nihon Shokakibyo Gakkai Zasshi. 2024. PMID: 38735750 Japanese.
-
An extremely rare case who underwent total remnant pancreatectomy due to recurrent pancreatic metastasis of intraductal tubulopapillary neoplasm.Clin J Gastroenterol. 2019 Apr;12(2):153-159. doi: 10.1007/s12328-018-0913-x. Epub 2018 Oct 4. Clin J Gastroenterol. 2019. PMID: 30284703
Cited by
-
Intraductal Tubulopapillary Neoplasm Diagnosed Before Surgery: A Case Report.Cureus. 2023 Mar 30;15(3):e36932. doi: 10.7759/cureus.36932. eCollection 2023 Mar. Cureus. 2023. PMID: 37131554 Free PMC article.
-
Total Pancreatectomy with Splenectomy for Multifocal Intraductal Tubulopapillary Neoplasm (ITPN) of the Pancreas Associated with Invasive Component: Report of a Rare Case.Am J Case Rep. 2020 Jul 10;21:e924760. doi: 10.12659/AJCR.924760. Am J Case Rep. 2020. PMID: 32647104 Free PMC article.
-
Intraductal tubulopapillary neoplasms of the pancreas and biliary tract: The black swan of hepatobiliary surgery.Ann Hepatobiliary Pancreat Surg. 2021 Nov 30;25(4):556-561. doi: 10.14701/ahbps.2021.25.4.556. Ann Hepatobiliary Pancreat Surg. 2021. PMID: 34845131 Free PMC article.
-
Imaging features of intraductal tubulopapillary neoplasm of the pancreas and its differentiation from conventional pancreatic ductal adenocarcinoma.Sci Rep. 2022 Sep 16;12(1):15557. doi: 10.1038/s41598-022-19517-6. Sci Rep. 2022. PMID: 36114217 Free PMC article.
-
Adenocarcinoma in Intraductal Tubulopapillary Neoplasm of the Pancreas: A Case Report and Literature Review.Cureus. 2023 Aug 5;15(8):e43006. doi: 10.7759/cureus.43006. eCollection 2023 Aug. Cureus. 2023. PMID: 37674950 Free PMC article.
References
-
- WHO, Bosman FT, Carneiro F, Hruban RH, et al. WHO classification of tumours of the digestive system. 2010.
-
- Yamaguchi H, Shimizu M, Ban S, et al. Intraductal tubulopapillary neoplasms of the pancreas distinct from pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms. Am J Surg Pathol 2009;33:1164–72. - PubMed
-
- Date K, Okabayashi T, Shima Y, et al. Clinicopathological features and surgical outcomes of intraductal tubulopapillary neoplasm of the pancreas: a systematic review. Langenbecks Arch Surg 2016;401:439–47. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
