

Measurement of Myofilament-Localized Calcium Dynamics in Adult Cardiomyocytes and the Effect of Hypertrophic Cardiomyopathy Mutations
- PMID: 30732532
- PMCID: PMC6485313
- DOI: 10.1161/CIRCRESAHA.118.314600
Measurement of Myofilament-Localized Calcium Dynamics in Adult Cardiomyocytes and the Effect of Hypertrophic Cardiomyopathy Mutations
Abstract
Rationale: Subcellular Ca2+ indicators have yet to be developed for the myofilament where disease mutation or small molecules may alter contractility through myofilament Ca2+ sensitivity. Here, we develop and characterize genetically encoded Ca2+ indicators restricted to the myofilament to directly visualize Ca2+ changes in the sarcomere.
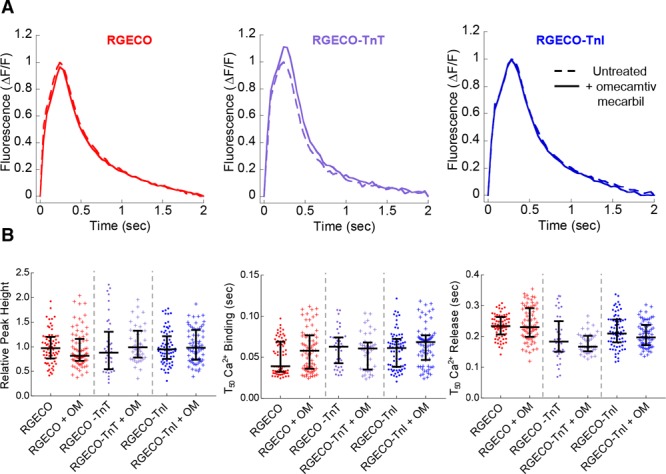
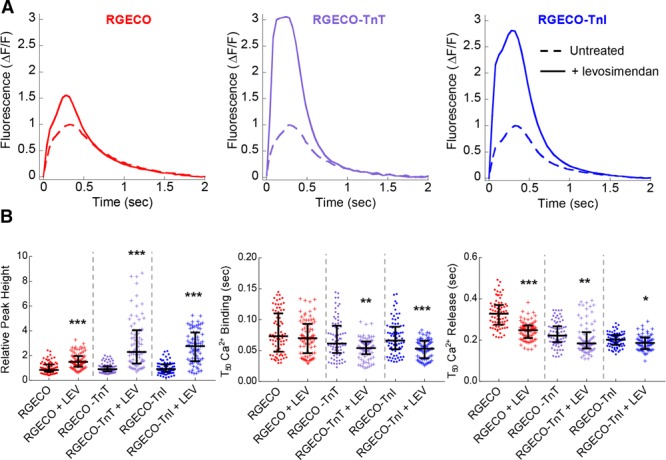
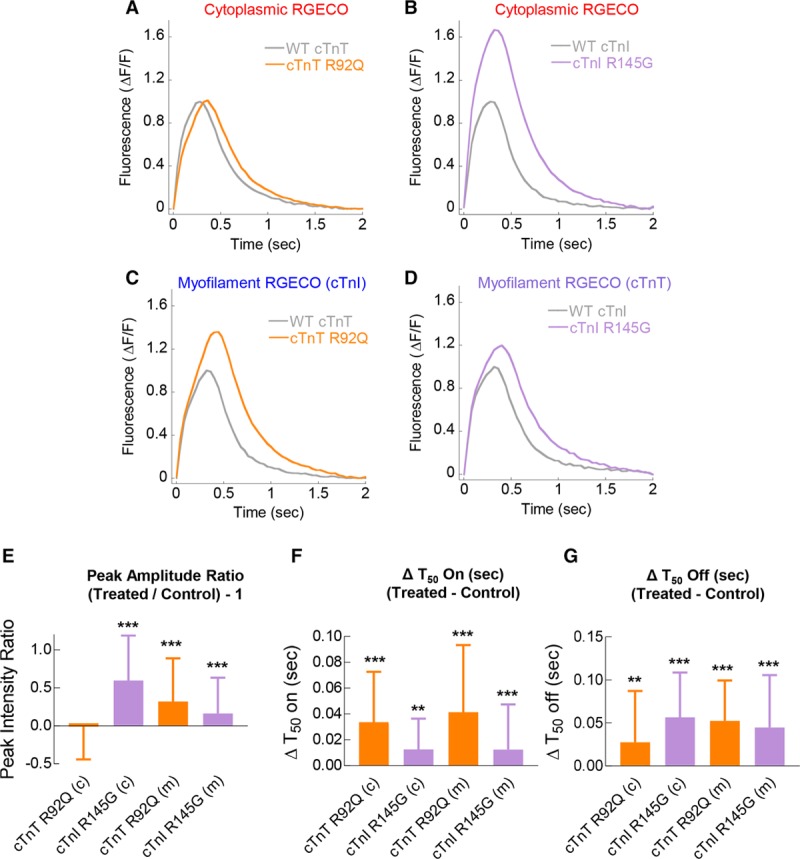
Objective: To produce and validate myofilament-restricted Ca2+ imaging probes in an adenoviral transduction adult cardiomyocyte model using drugs that alter myofilament function (MYK-461, omecamtiv mecarbil, and levosimendan) or following cotransduction of 2 established hypertrophic cardiomyopathy disease-causing mutants (cTnT [Troponin T] R92Q and cTnI [Troponin I] R145G) that alter myofilament Ca2+ handling.
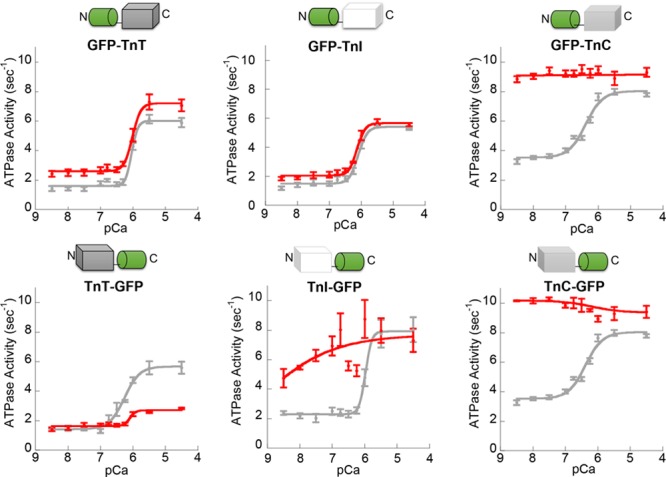
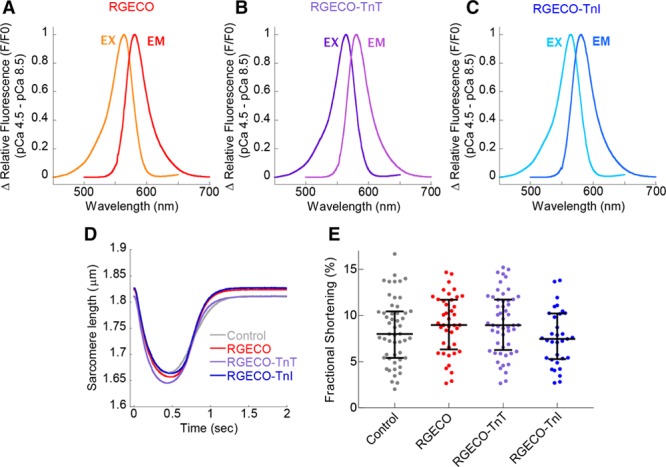
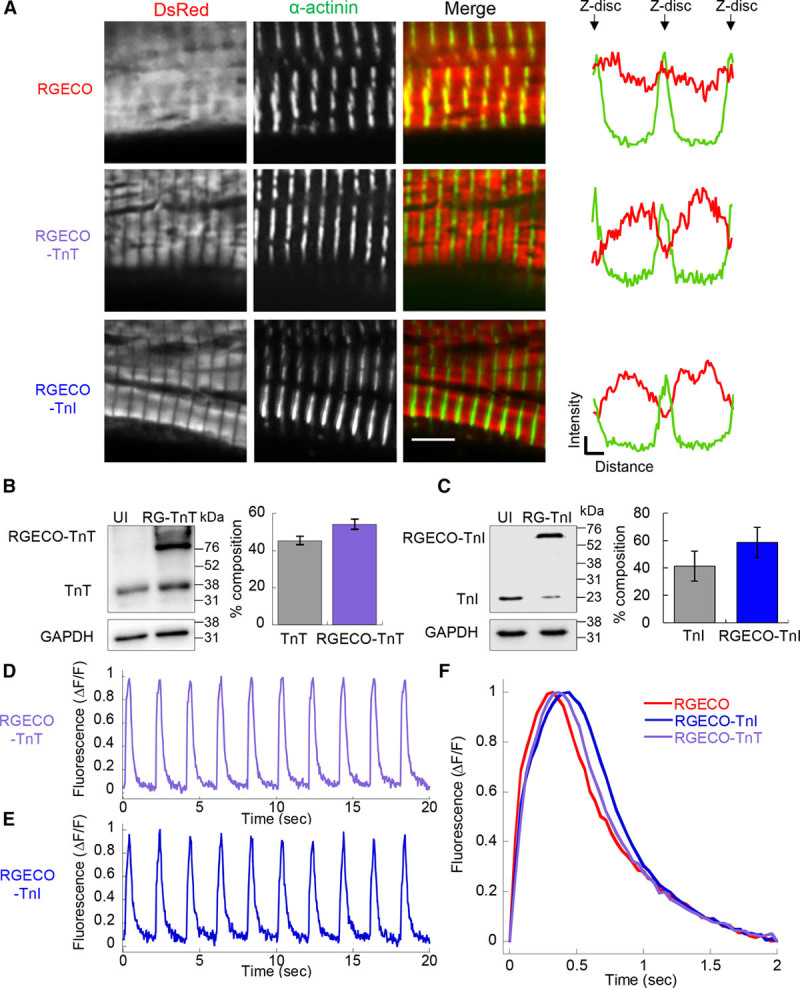
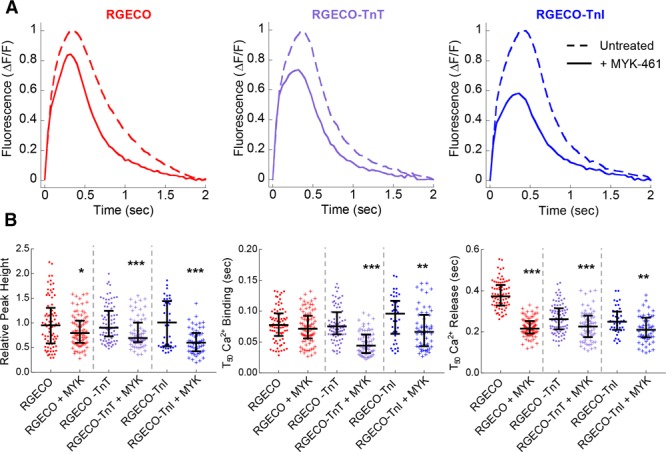
Methods and results: When expressed in adult ventricular cardiomyocytes RGECO-TnT (Troponin T)/TnI (Troponin I) sensors localize correctly to the sarcomere without contractile impairment. Both sensors report cyclical changes in fluorescence in paced cardiomyocytes with reduced Ca2+ on and increased Ca2+ off rates compared with unconjugated RGECO. RGECO-TnT/TnI revealed changes to localized Ca2+ handling conferred by MYK-461 and levosimendan, including an increase in Ca2+ binding rates with both levosimendan and MYK-461 not detected by an unrestricted protein sensor. Coadenoviral transduction of RGECO-TnT/TnI with hypertrophic cardiomyopathy causing thin filament mutants showed that the mutations increase myofilament [Ca2+] in systole, lengthen time to peak systolic [Ca2+], and delay [Ca2+] release. This contrasts with the effect of the same mutations on cytoplasmic Ca2+, when measured using unrestricted RGECO where changes to peak systolic Ca2+ are inconsistent between the 2 mutations. These data contrast with previous findings using chemical dyes that show no alteration of [Ca2+] transient amplitude or time to peak Ca2+.
Conclusions: RGECO-TnT/TnI are functionally equivalent. They visualize Ca2+ within the myofilament and reveal unrecognized aspects of small molecule and disease-associated mutations in living cells.
Keywords: calcium; cardiomyopathies; fluorescence; mutation; sarcomere.
Figures
Comment in
-
Sarcomere-Directed Calcium Reporters in Cardiomyocytes.Circ Res. 2019 Apr 12;124(8):1151-1153. doi: 10.1161/CIRCRESAHA.119.314877. Circ Res. 2019. PMID: 30973804 Free PMC article. No abstract available.
References
-
- Maron BJ, Gardin JM, Flack JM, Gidding SS, Kurosaki TT, Bild DE. Prevalence of hypertrophic cardiomyopathy in a general population of young adults. Echocardiographic analysis of 4111 subjects in the CARDIA Study. Coronary Artery Risk Development in (Young) Adults. Circulation. 1995;92:785–789. - PubMed
-
- Watkins H, Ashrafian H, Redwood C. Inherited cardiomyopathies. N Engl J Med. 2011;364:1643–1656. doi: 10.1056/NEJMra0902923. - PubMed
-
- Redwood CS, Moolman-Smook JC, Watkins H. Properties of mutant contractile proteins that cause hypertrophic cardiomyopathy. Cardiovasc Res. 1999;44:20–36. - PubMed
-
- Knollmann BC, Kirchhof P, Sirenko SG, Degen H, Greene AE, Schober T, Mackow JC, Fabritz L, Potter JD, Morad M. Familial hypertrophic cardiomyopathy-linked mutant troponin T causes stress-induced ventricular tachycardia and Ca2+-dependent action potential remodeling. Circ Res. 2003;92:428–436. doi: 10.1161/01.RES.0000059562.91384.1A. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
