

On the estimation of population cause-specific mortality fractions from in-hospital deaths
- PMID: 30732593
- PMCID: PMC6367755
- DOI: 10.1186/s12916-019-1267-z
On the estimation of population cause-specific mortality fractions from in-hospital deaths
Abstract
Background: Almost all countries without complete vital registration systems have data on deaths collected by hospitals. However, these data have not been widely used to estimate cause of death (COD) patterns in populations because only a non-representative fraction of people in these countries die in health facilities. Methods that can exploit hospital mortality statistics to reliably estimate community COD patterns are required to strengthen the evidence base for disease and injury control programs. We propose a method that weights hospital-certified causes by the probability of death to estimate population cause-specific mortality fractions (CSMFs).
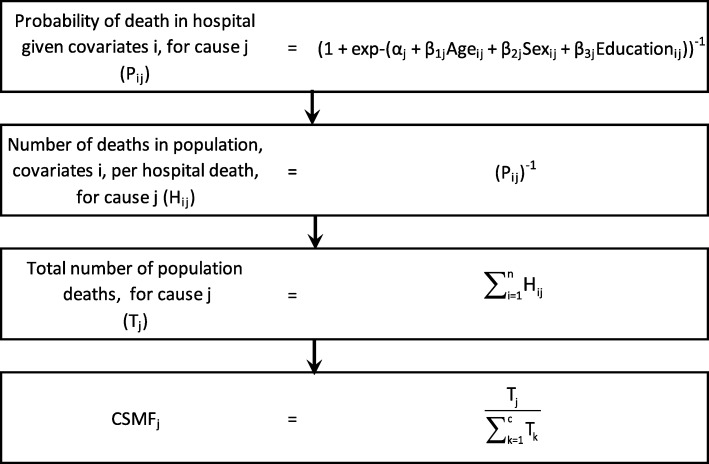
Methods: We used an established verbal autopsy instrument (VAI) to collect data from hospital catchment areas in Chandpur and Comilla Districts, Bangladesh, and Bohol province, the Philippines, between 2011 and 2014, along with demographic covariates for each death. Hospital medical certificates of cause of death (death certificates) were collected and mapped to the corresponding cause categories of the VAI. Tariff 2.0 was used to assign a COD for community deaths. Logistic regression models were created for broad causes in each country to calculate the probability of in-hospital death, given a set of covariate values. The reweighted CSMFs for deaths in the hospital catchment population, represented by each hospital death, were calculated from the corresponding regression models.
Results: We collected data on 4228 adult deaths in the Philippines and 3725 deaths in Bangladesh. Short time to hospital and education were consistently associated with in-hospital death in the Philippines and absence of a disability was consistently associated with in-hospital death in Bangladesh. Non-communicable diseases (excluding stroke) and stroke were the leading causes of death in both the Philippines (33.9%, 19.1%) and Bangladesh (46.1%, 21.1%) according to the reweighted method. The reweighted method generally estimated CSMFs that fell between those derived from hospitals and those diagnosed by Tariff 2.0.
Conclusions: Statistical methods can be used to derive estimates of cause-specific probability of death in-hospital for Bangladesh and the Philippines to generate population CSMFs. In regions where hospital death certification is of reasonable quality and routine verbal autopsy is not applied, these estimates could be applied to generate cost-effective and robust CSMFs for the population.
Keywords: Bangladesh; Cause of death; Death certificate; Philippines; Vital registration.
Conflict of interest statement
Ethics approval and consent to participate
The methods of this study were approved by the Medical Research Ethics Committee of the University of Queensland, Australia; the Institutional Review Board of the Research Institute of Tropical Medicine, Philippines; and the Ethical Review Committee of the International Centre for Diarrhoeal Disease Research, Bangladesh. All data were collected with informed verbal consent from participants before beginning the interview. This method of consent was approved by the review boards at each site.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- English M, Mwaniki P, Julius T, Chepkirui M, Gathara D, Ouma PO, et al. Hospital mortality – a neglected but rich source of information supporting the transition to higher quality health systems in low and middle income countries. BMC Med. 2018;16:32. doi: 10.1186/s12916-018-1024-8. - DOI - PMC - PubMed
-
- Rampatige R, Gamage S, Peiris S, Lopez AD. Assessing the reliability of causes of death reported by the vital registration system in Sri Lanka: medical records review in Colombo. Health Inf Manag. 2013;42:20–28. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
