

SGLT2 inhibition with empagliflozin improves coronary microvascular function and cardiac contractility in prediabetic ob/ob-/- mice
- PMID: 30732594
- PMCID: PMC6366096
- DOI: 10.1186/s12933-019-0820-6
SGLT2 inhibition with empagliflozin improves coronary microvascular function and cardiac contractility in prediabetic ob/ob-/- mice
Abstract
Background: Sodium-glucose cotransporter 2 inhibitors (SGLT2i) is the first class of anti-diabetes treatment that reduces mortality and risk for hospitalization due to heart failure. In clinical studies it has been shown that SGLT2i's promote a general shift to fasting state metabolism characterized by reduced body weight and blood glucose, increase in glucagon/insulin ratio and modest increase in blood ketone levels. Therefore, we investigated the connection between metabolic changes and cardiovascular function in the ob/ob-/- mice; a rodent model of early diabetes with specific focus on coronary microvascular function. Due to leptin deficiency these mice develop metabolic syndrome/diabetes and hepatic steatosis. They also develop cardiac contractile and microvascular dysfunction and are thus a promising model for translational studies of cardiometabolic diseases. We investigated whether this mouse model responded in a human-like manner to empagliflozin treatment in terms of metabolic parameters and tested the hypothesis that it could exert direct effects on coronary microvascular function and contractile performance.
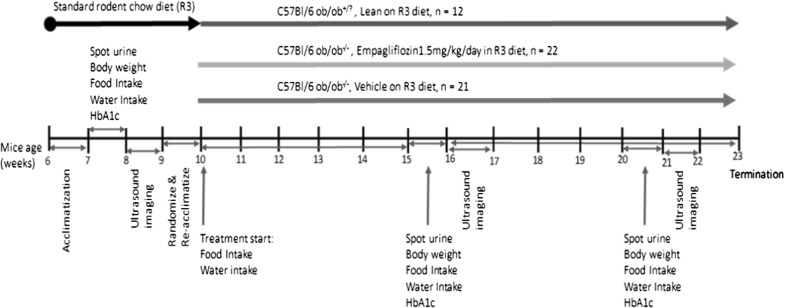
Methods: Lean, ob/ob-/- untreated and ob/ob-/- treated with SGLT2i were followed for 10 weeks. Coronary flow velocity reserve (CFVR) and fractional area change (FAC) were monitored with non-invasive Doppler ultrasound imaging. Food intake, urinary glucose excursion and glucose control via HbA1c measurements were followed throughout the study. Liver steatosis was assessed by histology and metabolic parameters determined at the end of the study.
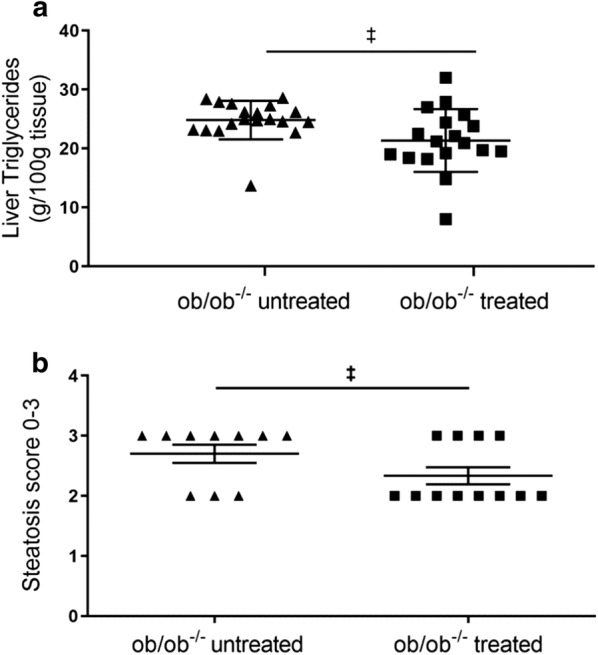
Results: Sodium-glucose cotransporter 2 inhibitors treatment of ob/ob-/- animals resulted in a switch to a more catabolic state as observed in clinical studies: blood cholesterol and HbA1c were decreased whereas glucagon/insulin ratio and ketone levels were increased. SGLT2i treatment reduced liver triglyceride, steatosis and alanine aminotransferase, an indicator for liver dysfunction. L-Arginine/ADMA ratio, a marker for endothelial function was increased. SGLT2i treatment improved both cardiac contractile function and coronary microvascular function as indicated by improvement of FAC and CFVR, respectively.
Conclusions: Sodium-glucose cotransporter 2 inhibitors treatment of ob/ob-/- mice mimics major clinical findings regarding metabolism and cardiovascular improvements and is thus a useful translational model. We demonstrate that SGLT2 inhibition improves coronary microvascular function and contractile performance, two measures with strong predictive values in humans for CV outcome, alongside with the known metabolic changes in a preclinical model for prediabetes and heart failure.
Keywords: Coronary; Endothelial; Microvascular; Prediabetes; SGLT2.
Figures





References
-
- Luscher TF, Creager MA, Beckman JA, Cosentino F. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part II. Circulation. 2003;108(13):1655–1661. - PubMed
-
- Salazar MR, Carbajal HA, Espeche WG, Aizpurua M, Leiva Sisnieguez CE, Leiva Sisnieguez BC, Stavile RN, March CE, Reaven GM. Insulin resistance: the linchpin between prediabetes and cardiovascular disease. Diabetes Vasc Dis Res. 2016;13(2):157–163. - PubMed
-
- Zhuo X, Zhang P, Hoerger TJ. Lifetime direct medical costs of treating type 2 diabetes and diabetic complications. Am J Prev Med. 2013;45(3):253–261. - PubMed
-
- Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–2128. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
