

Assessment of patients' self-perceived intensive care unit discomforts: Validation of the 18-item version of the IPREA
- PMID: 30732654
- PMCID: PMC6367827
- DOI: 10.1186/s12955-019-1101-5
Assessment of patients' self-perceived intensive care unit discomforts: Validation of the 18-item version of the IPREA
Abstract
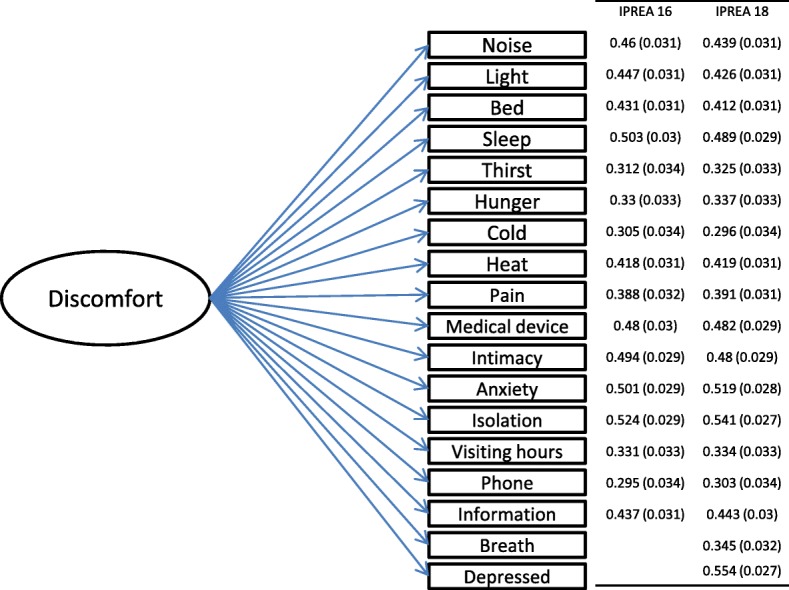
Background and aims: We reported the validation of the 18-item version of the 'Inconforts des Patients de REAnimation (IPREA)' questionnaire that includes 2 new items exploring feeling depressed and shortness of breath during an intensive care unit (ICU) stay.
Methods: The validation process was integrated in a multicenter, cluster-randomized, controlled, two-parallel group study built to assess the effectiveness of a tailored multicomponent program for reducing self-perceived discomfort in the ICU. All patients aged 18 years or older who survived an ICU stay of 3 calendar days or more were eligible for inclusion. Data collection included demographics (sex, age), type of admission (medical and surgical), health status scores at admission (Knaus score and McCabe index, Simplified Acute Physiology Score (SAPS) II), specific ICU therapeutics such as mechanical ventilation (MV), noninvasive ventilation (NIV), use of vasopressors, or renal replacement therapy (RRT), and ICU stay duration.
Results: A total of 994 patients were included. The initial structure of IPREA was confirmed using confirmatory factor analysis showing satisfactory fit (RMSEA at 0.042, CFI at 0.912). No multidimensional structure was identified, allowing the calculation of an overall discomfort score. The three highest discomforts were sleep deprivation, thirst, and perfusion lines and other devices, and the 3 lowest discomforts were limited visiting hours, hunger, and isolation. The overall discomfort score of the 18-item version of IPREA did not differ between men and women. Higher age was significantly correlated with a lower overall discomfort score. While MV was not linked to self-reported discomfort, patients treated by NIV reported higher overall discomfort scores than patients not treated by NIV.
Conclusion: The 18-item version of IPREA is easy to use and possesses satisfactory psychometric properties. The availability of a reliable and valid French questionnaire asking about patients' self-perceived ICU discomforts enables feedback from the health care team to be incorporated in a continuous quality health care improvement strategy.
Trial registration: clinicaltrial.gov NCT02442934 (registration date: May 18, 2015, retrospectively registered).
Keywords: Critical care; Discomfort; IPREA; Questionnaire; Validation.
Conflict of interest statement
Ethics approval and consent to participate
Regulatory monitoring has been performed in accordance with the French law needing the approval of the French ethics committee (Comité de Protection des Personnes Tours Région Centre-Ouest 1, 28/08/2013, reference number 2013-S10). All records and subjects’ identity remained confidential in accordance with the French regulations: the French National Committee of Informatics and Liberties (Commission nationale de l’informatique et des libertés, 20/03/2014, reference number DR-2014-097) and the French Consultative Committee for the data processing in health research (Comité consultatif sur le traitement de l’information en matière de recherche dans le domaine de la santé, 12/12/2013, reference number 13.642bis). Consent has been obtained from each participant.
Consent for publication
Not applicable.
Competing interests
Dr. Kalfon received consulting fees from Philips Healthcare. On behalf of all remaining authors, the corresponding author states that the remaining authors have no conflict of interest. The other authors have stated that they had no interests which might be perceived as posing a conflict or bias.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Puntillo KA, Max A, Timsit JF, Vignoud L, Chanques G, Robleda G, et al. Determinants of procedural pain intensity in the intensive care unit. The Europain(R) study. Am J Respir Crit Care Med. 2014;189:39–47. - PubMed
-
- Bruera E, Kuehn N, Miller MJ, Selmser P, Macmillan K. The Edmonton symptom assessment system (ESAS): a simple method for the assessment of palliative care patients. J Palliat Care. 1991;7:6–9. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
