

Direct Current Cardioversion of Atrial Arrhythmias in Adults With Cardiac Amyloidosis
- PMID: 30732713
- PMCID: PMC6378685
- DOI: 10.1016/j.jacc.2018.10.079
Direct Current Cardioversion of Atrial Arrhythmias in Adults With Cardiac Amyloidosis
Abstract
Background: Arrhythmias, conduction abnormalities, and intracardiac thrombus are common in patients with cardiac amyloidosis (CA). Outcomes of direct-current cardioversion (DCCV) for atrial arrhythmias in patients with CA are unknown.
Objectives: This study sought to examine DCCV procedural outcomes in patients with CA.
Methods: Patients with CA scheduled for DCCV for atrial arrhythmias from January 2000 through December 2012 were identified and matched 2:1 with control patients by age, sex, type of atrial arrhythmia, and date of DCCV.
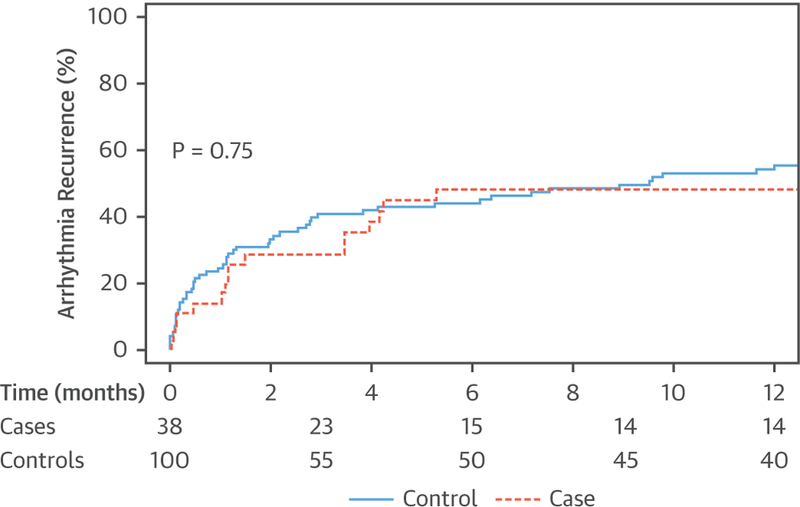
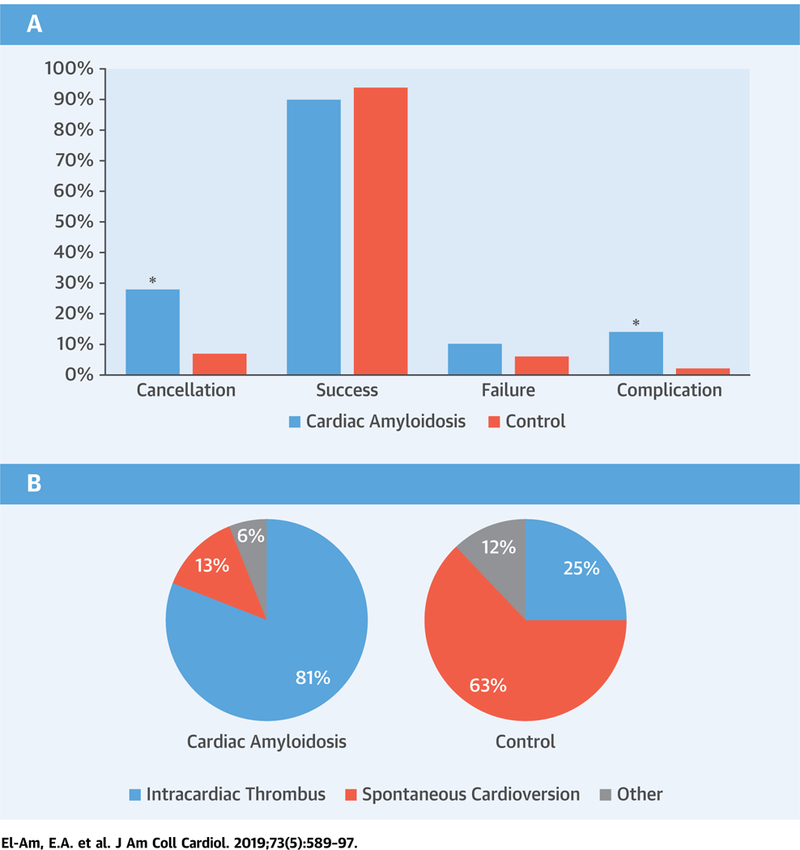
Results: CA patients (n = 58, mean age 69 ± 9 years, 81% male) were included. CA patients had a significantly higher cardioversion cancellation rate (28% vs. 7%; p < 0.001) compared with control patients, mainly due to intracardiac thrombus identified on transesophageal echocardiogram (13 of 16 [81%] vs. 2 of 8 [25%]; p = 0.02); 4 of 13 of the CA patients (31%) with intracardiac thrombus on transesophageal echocardiogram received adequate anticoagulation ≥3 weeks and another 2 of 13 (15%) had arrhythmia duration <48 h. DCCV success rate (90% vs. 94%; p = 0.4) was not different. Procedural complications were more frequent in CA versus control patients (6 of 42 [14%] vs. 2 of 106 [2%]; p = 0.007); complications in CA included ventricular arrhythmias in 2 and severe bradyarrhythmias requiring pacemaker implantation in 2. The only complication in the control group was self-limited bradyarrhythmias.
Conclusions: Patients with CA undergoing DCCV had a significantly high cancellation rate mainly due to a high incidence of intracardiac thrombus even among patients who received adequate anticoagulation. Although the success rate of restoring sinus rhythm was high, tachyarrhythmias and bradyarrhythmias complicating DCCV were significantly more frequent in CA patients compared with control patients.
Keywords: atrial arrhythmia; atrial fibrillation; cardiac amyloidosis; cardioversion; intracardiac thrombus; transesophageal echocardiogram.
Copyright © 2019 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Cardiac Amyloidosis and the Risks of Cardioversion.J Am Coll Cardiol. 2019 Feb 12;73(5):598-601. doi: 10.1016/j.jacc.2018.10.080. J Am Coll Cardiol. 2019. PMID: 30732714 No abstract available.
-
Cardiac Amyloidosis and Electrical Cardioversion: Is the Thrombus There or Not?J Am Coll Cardiol. 2019 Jun 11;73(22):2909-2910. doi: 10.1016/j.jacc.2019.03.491. J Am Coll Cardiol. 2019. PMID: 31171103 No abstract available.
-
Predicting the Unpredictable: How to Score the Risk of Stroke in Cardiac Amyloidosis?J Am Coll Cardiol. 2019 Jun 11;73(22):2910-2911. doi: 10.1016/j.jacc.2019.02.078. J Am Coll Cardiol. 2019. PMID: 31171104 No abstract available.
-
Reply: Cardiac Amyloidosis, Atrial Arrhythmias, Thrombus, and Stroke: A Vexing Problem.J Am Coll Cardiol. 2019 Jun 11;73(22):2911-2913. doi: 10.1016/j.jacc.2019.04.005. J Am Coll Cardiol. 2019. PMID: 31171105 No abstract available.
References
-
- Falk RH, Comenzo RL, Skinner M. The systemic amyloidoses. N Engl J Med 1997;337:898–909. - PubMed
-
- Kyle RA, Linos A, Beard CM, et al. Incidence and natural history of primary systemic amyloidosis in Olmsted County, Minnesota, 1950 through 1989. Blood 1992;79:1817–22. - PubMed
-
- Rapezzi C, Merlini G, Quarta CC, et al. Systemic cardiac amyloidoses: disease profiles and clinical courses of the 3 main types. Circulation 2009;120: 1203–12. - PubMed
-
- Falk RH. Diagnosis and management of the cardiac amyloidoses. Circulation 2005;112: 2047–60. - PubMed
-
- Lachmann HJ, Goodman HJ, Gilbertson JA, et al. Natural history and outcome in systemic AA amyloidosis. N Engl J Med 2007;356:2361–71. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
