

Imaging and Impact of Myocardial Fibrosis in Aortic Stenosis
- PMID: 30732723
- PMCID: PMC6361867
- DOI: 10.1016/j.jcmg.2018.11.026
Imaging and Impact of Myocardial Fibrosis in Aortic Stenosis
Abstract
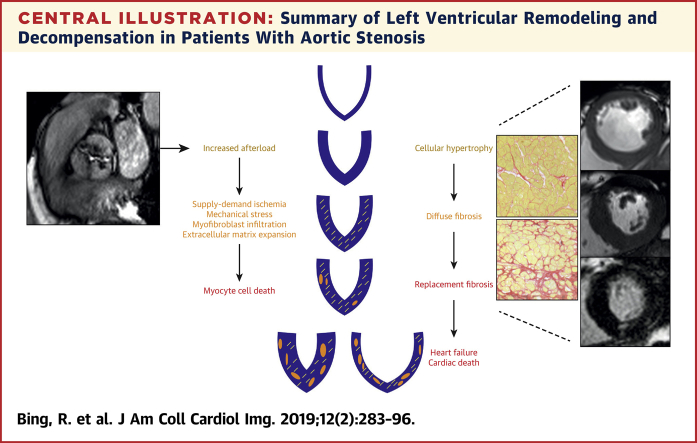
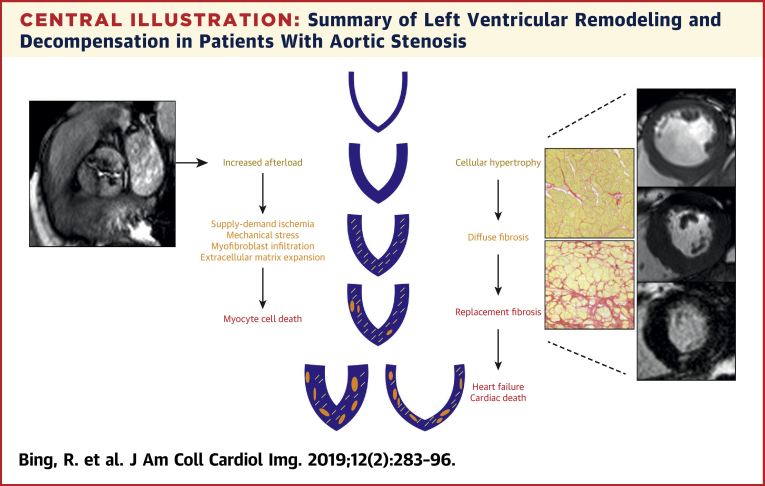
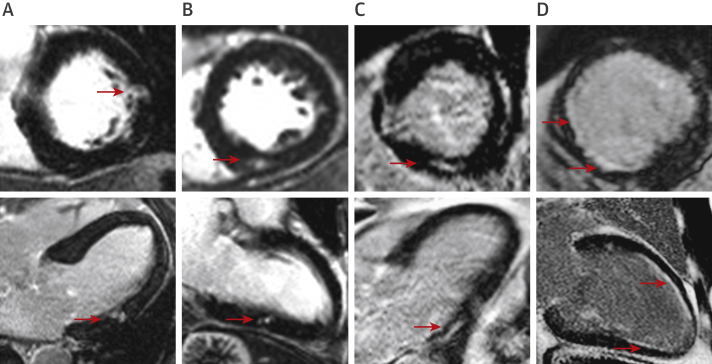
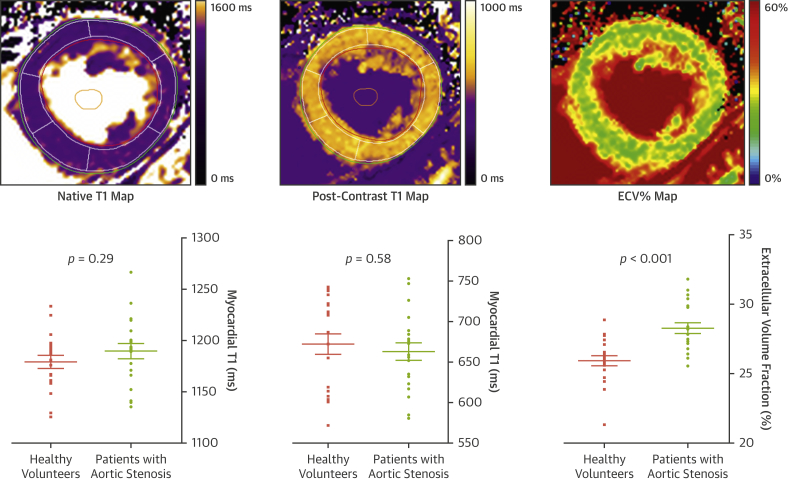
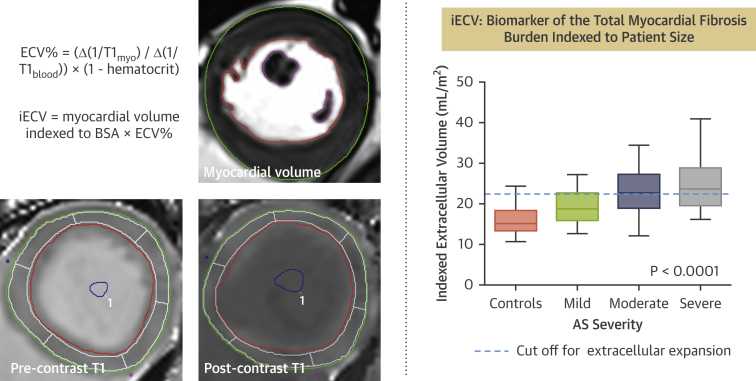
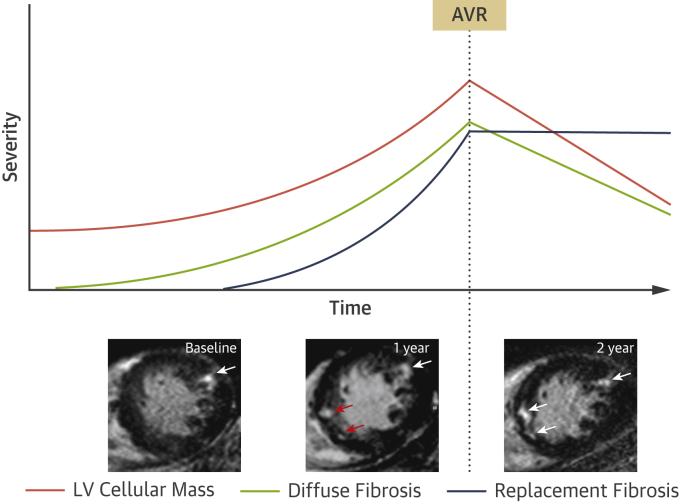
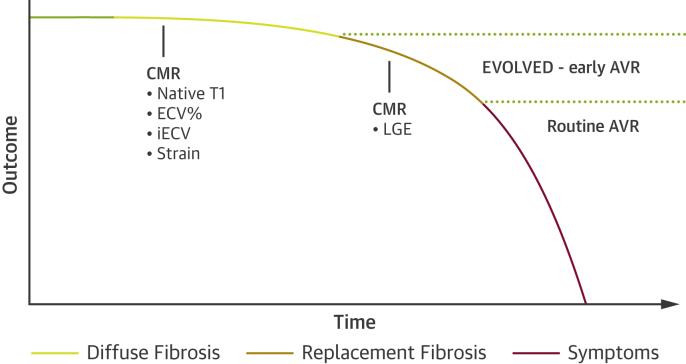
Aortic stenosis is characterized both by progressive valve narrowing and the left ventricular remodeling response that ensues. The only effective treatment is aortic valve replacement, which is usually recommended in patients with severe stenosis and evidence of left ventricular decompensation. At present, left ventricular decompensation is most frequently identified by the development of typical symptoms or a marked reduction in left ventricular ejection fraction <50%. However, there is growing interest in using the assessment of myocardial fibrosis as an earlier and more objective marker of left ventricular decompensation, particularly in asymptomatic patients, where guidelines currently rely on nonrandomized data and expert consensus. Myocardial fibrosis has major functional consequences, is the key pathological process driving left ventricular decompensation, and can be divided into 2 categories. Replacement fibrosis is irreversible and identified using late gadolinium enhancement on cardiac magnetic resonance, while diffuse fibrosis occurs earlier, is potentially reversible, and can be quantified with cardiac magnetic resonance T1 mapping techniques. There is a substantial body of observational data in this field, but there is now a need for randomized clinical trials of myocardial imaging in aortic stenosis to optimize patient management. This review will discuss the role that myocardial fibrosis plays in aortic stenosis, how it can be imaged, and how these approaches might be used to track myocardial health and improve the timing of aortic valve replacement.
Keywords: T(1) mapping; aortic stenosis; cardiac magnetic resonance; late gadolinium enhancement; myocardial fibrosis.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Nkomo V.T., Gardin J.M., Skelton T.N., Gottdiener J.S., Scott C.G., Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368:1005–1011. - PubMed
-
- Iung B., Vahanian A. Epidemiology of valvular heart disease in the adult. Nat Rev Cardiol. 2011;8:162–172. - PubMed
-
- Osnabrugge R.L., Mylotte D., Head S.J. Aortic stenosis in the elderly: disease prevalence and number of candidates for transcatheter aortic valve replacement: a meta-analysis and modeling study. J Am Coll Cardiol. 2013;62:1002–1012. - PubMed
-
- Dweck M.R., Boon N.A., Newby D.E. Calcific aortic stenosis: a disease of the valve and the myocardium. J Am Coll Cardiol. 2012;60:1854–1863. - PubMed
-
- Rosenhek R., Zilberszac R., Schemper M. Natural history of very severe aortic stenosis. Circulation. 2010;121:151–156. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
