

Arthroscopic hip surgery compared with physiotherapy and activity modification for the treatment of symptomatic femoroacetabular impingement: multicentre randomised controlled trial
- PMID: 30733197
- PMCID: PMC6365841
- DOI: 10.1136/bmj.l185
Arthroscopic hip surgery compared with physiotherapy and activity modification for the treatment of symptomatic femoroacetabular impingement: multicentre randomised controlled trial
Erratum in
-
Correction for vol. 372, p.BMJ. 2021 Jan 18;372:m3715. doi: 10.1136/bmj.m3715. BMJ. 2021. PMID: 33461966 Free PMC article.
Abstract
Objective: To compare arthroscopic hip surgery with physiotherapy and activity modification for improving patient reported outcome measures in patients with symptomatic femoroacetabular impingement (FAI).
Design: Two group parallel, assessor blinded, pragmatic randomised controlled trial.
Setting: Secondary and tertiary care centres across seven NHS England sites.
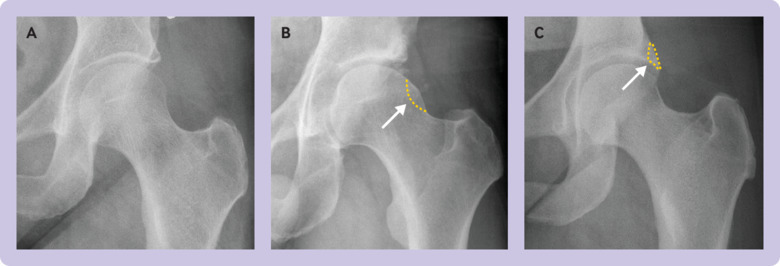
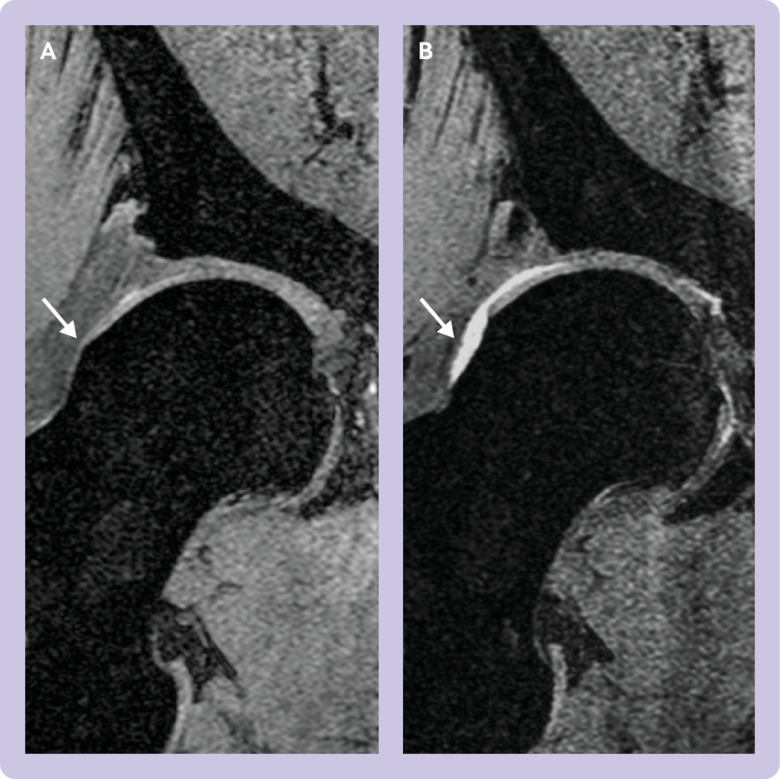
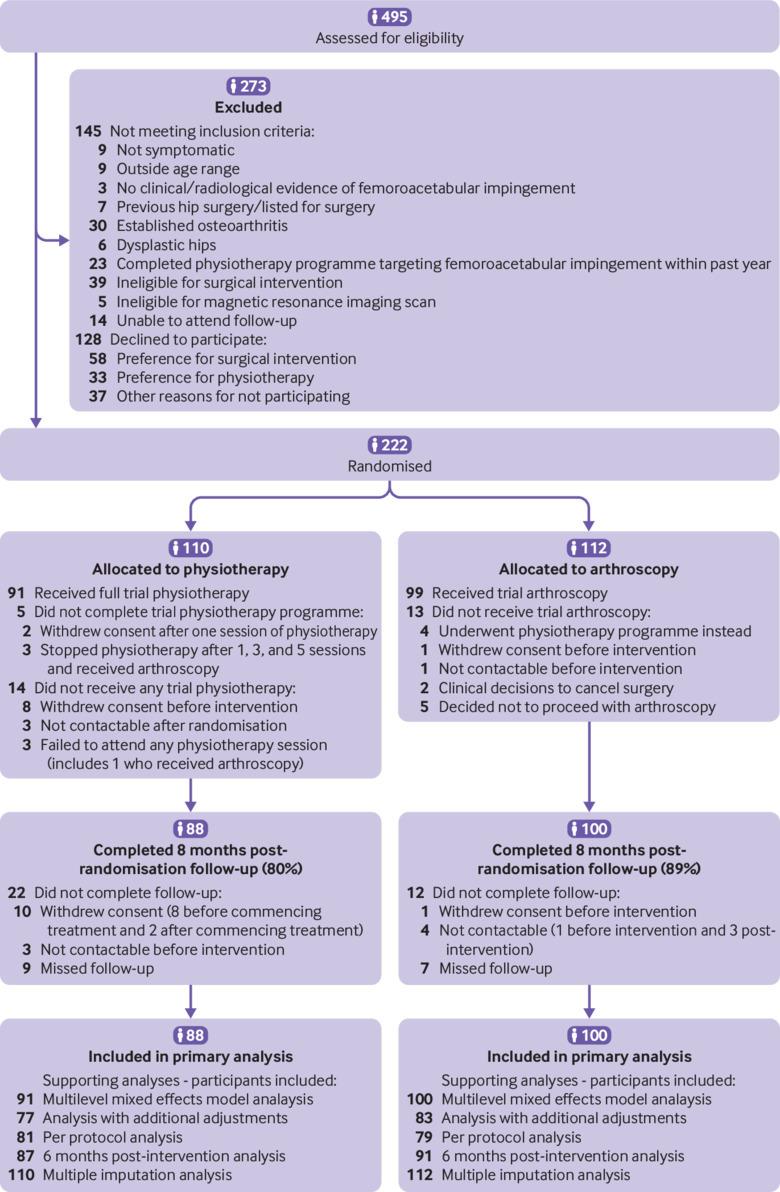
Participants: 222 participants aged 18 to 60 years with symptomatic FAI confirmed clinically and with imaging (radiography or magnetic resonance imaging) were randomised (1:1) to receive arthroscopic hip surgery (n=112) or a programme of physiotherapy and activity modification (n=110). Exclusion criteria included previous surgery, completion of a physiotherapy programme targeting FAI within the preceding 12 months, established osteoarthritis (Kellgren-Lawrence grade ≥2), and hip dysplasia (centre-edge angle <20 degrees).
Interventions: Participants in the physiotherapy group received a goal based programme tailored to individual patient needs, with emphasis on improving core stability and movement control. A maximum of eight physiotherapy sessions were delivered over five months. Participants in the arthroscopic surgery group received surgery to excise the bone that impinged during hip movements, followed by routine postoperative care.
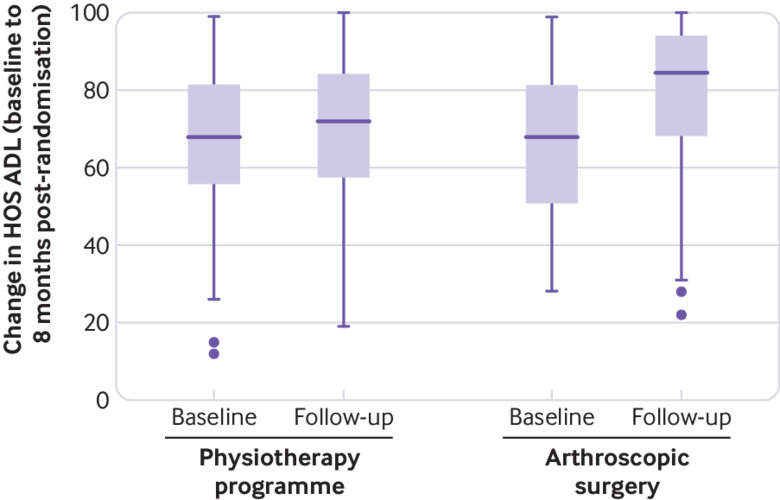
Main outcome measures: The primary outcome measure was the hip outcome score activities of daily living subscale (HOS ADL) at eight months post-randomisation, with a minimum clinically important difference between groups of 9 points. Secondary outcome measures included additional patient reported outcome measures and clinical assessment.
Results: At eight months post-randomisation, data were available for 100 patients in the arthroscopic hip surgery group (89%) and 88 patients in the physiotherapy programme group (80%). Mean HOS ADL was 78.4 (95% confidence interval 74.4 to 82.3) for patients randomised to arthroscopic hip surgery and 69.2 (65.2 to 73.3) for patients randomised to the physiotherapy programme. After adjusting for baseline HOS ADL, age, sex, and study site, the mean HOS ADL was 10.0 points higher (6.4 to 13.6) in the arthroscopic hip surgery group compared with the physiotherapy programme group (P<0.001)). No serious adverse events were reported in either group.
Conclusions: Patients with symptomatic FAI referred to secondary or tertiary care achieve superior outcomes with arthroscopic hip surgery than with physiotherapy and activity modification.
Trial registration: ClinicalTrials.gov NCT01893034.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from Arthritis Research UK and NIHR Oxford Biomedical Research Centre for the submitted work. The researchers and funders were independent. AJRP received funding from the Royal College of Surgeons of England and Dunhill Medical Trust. Unrelated to the submitted work, VK received support from Stryker and Smith and Nephew for educational consultancy, AA received support from Stryker, Smith and Nephew, and Zimmer Biomet for lectures, and SGJ received research grants and fees for lectures from Zimmer Biomet, Corin, and ConMed, and research grants from Neurotechnics, Johnson and Johnson, and Siemens.
Figures
Comment in
-
In Symptomatic Femoroacetabular Impingement, Arthroscopic Hip Surgery Improved Outcomes at 8 Months Compared with Physiotherapy and Activity Modification.J Bone Joint Surg Am. 2019 Nov 20;101(22):2062. doi: 10.2106/JBJS.19.00986. J Bone Joint Surg Am. 2019. PMID: 31764370 No abstract available.
-
Critically appraised paper: Arthroscopic hip surgery was superior to physiotherapy and activity modification in patients with femoroacetabular impingement [commentary].J Physiother. 2020 Apr;66(2):130. doi: 10.1016/j.jphys.2020.02.010. Epub 2020 Apr 11. J Physiother. 2020. PMID: 32291216 No abstract available.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical