

Challenges to curing primary brain tumours
- PMID: 30733593
- PMCID: PMC6650350
- DOI: 10.1038/s41571-019-0177-5
Challenges to curing primary brain tumours
Abstract
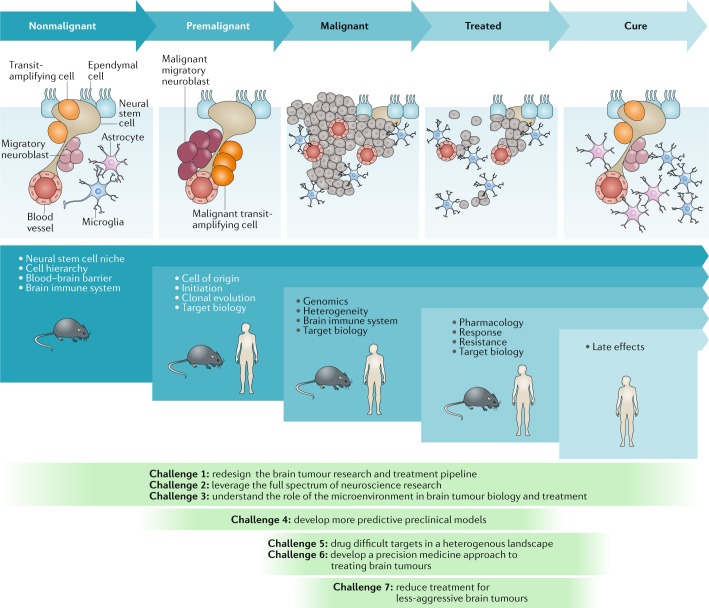
Despite decades of research, brain tumours remain among the deadliest of all forms of cancer. The ability of these tumours to resist almost all conventional and novel treatments relates, in part, to the unique cell-intrinsic and microenvironmental properties of neural tissues. In an attempt to encourage progress in our understanding and ability to successfully treat patients with brain tumours, Cancer Research UK convened an international panel of clinicians and laboratory-based scientists to identify challenges that must be overcome if we are to cure all patients with a brain tumour. The seven key challenges summarized in this Position Paper are intended to serve as foci for future research and investment.
Conflict of interest statement
P.W. and R.C. are employees of The Institute of Cancer Research (ICR), which has a commercial interest in a range of drug targets. The ICR operates a Rewards to Inventors scheme whereby employees of the ICR may receive financial benefit following commercial licensing of a project. P.W. is a consultant/scientific advisory board member for NextechInvest, Storm Therapeutics, Astex Pharmaceuticals and CV6 and holds stock in Chroma Therapeutics, NextInvest and Storm Therapeutics; he is also a Non-Executive Director of Storm Therapeutics and the Royal Marsden NHS Trust and a Director of the non-profit Chemical Probes Portal. R.C. is an advisor to Syncona Limited and holds equity in Celgene Corporation, e-Therapeutics and Monte Rosa Therapeutics. The other authors declare no competing interests.
Figures
Comment in
-
Reply to 'Assembling the brain trust: the multidisciplinary imperative in neuro-oncology'.Nat Rev Clin Oncol. 2019 Aug;16(8):522-523. doi: 10.1038/s41571-019-0236-y. Nat Rev Clin Oncol. 2019. PMID: 31150022 No abstract available.
-
Assembling the brain trust: the multidisciplinary imperative in neuro-oncology.Nat Rev Clin Oncol. 2019 Aug;16(8):521-522. doi: 10.1038/s41571-019-0235-z. Nat Rev Clin Oncol. 2019. PMID: 31150024 No abstract available.
References
-
- Chinot OL, et al. Bevacizumab plus radiotherapy–temozolomide for newly diagnosed glioblastoma. N. Engl. J. Med. 2014;370:709–722. - PubMed
-
- Chemaitilly W, Armstrong GT, Gajjar A, Hudson MM. Hypothalamic-pituitary axis dysfunction in survivors of childhood CNS tumors: importance of systematic follow-up and early endocrine consultation. J. Clin. Oncol. 2016;34:4315–4319. - PubMed
Publication types
MeSH terms
Grants and funding
- 28667/CRUK_/Cancer Research UK/United Kingdom
- 28028/CRUK_/Cancer Research UK/United Kingdom
- R01 CA116659/CA/NCI NIH HHS/United States
- 27413/CRUK_/Cancer Research UK/United Kingdom
- 26398/CRUK_/Cancer Research UK/United Kingdom
- 15958/CRUK_/Cancer Research UK/United Kingdom
- 28289/CRUK_/Cancer Research UK/United Kingdom
- R01 NS089272/NS/NINDS NIH HHS/United States
- Z99 CA999999/ImNIH/Intramural NIH HHS/United States
- R01 CA129958/CA/NCI NIH HHS/United States
- MC_PC_12009/MRC_/Medical Research Council/United Kingdom
- 22897/CRUK_/Cancer Research UK/United Kingdom
- 17368/CRUK_/Cancer Research UK/United Kingdom
- P30 CA008748/CA/NCI NIH HHS/United States
- 21992/CRUK_/Cancer Research UK/United Kingdom
- K02 NS047409/NS/NINDS NIH HHS/United States
- 17242/CRUK_/Cancer Research UK/United Kingdom
- P30 CA014236/CA/NCI NIH HHS/United States
- P01 CA096832/CA/NCI NIH HHS/United States
- 22492/CRUK_/Cancer Research UK/United Kingdom
- R35 CA197718/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
