

Early Mortality in Patients With Muscle-Invasive Bladder Cancer Undergoing Cystectomy in the United States
- PMID: 30734024
- PMCID: PMC6349610
- DOI: 10.1093/jncics/pky075
Early Mortality in Patients With Muscle-Invasive Bladder Cancer Undergoing Cystectomy in the United States
Abstract
Background: Although radical cystectomy (RC) is a standard treatment for muscle-invasive bladder cancer (MIBC), for many patients the risks versus benefits of RC may favor other approaches. We sought to define the landscape of early postcystectomy mortality in the United States and identify patients at high risk using pretreatment variables.
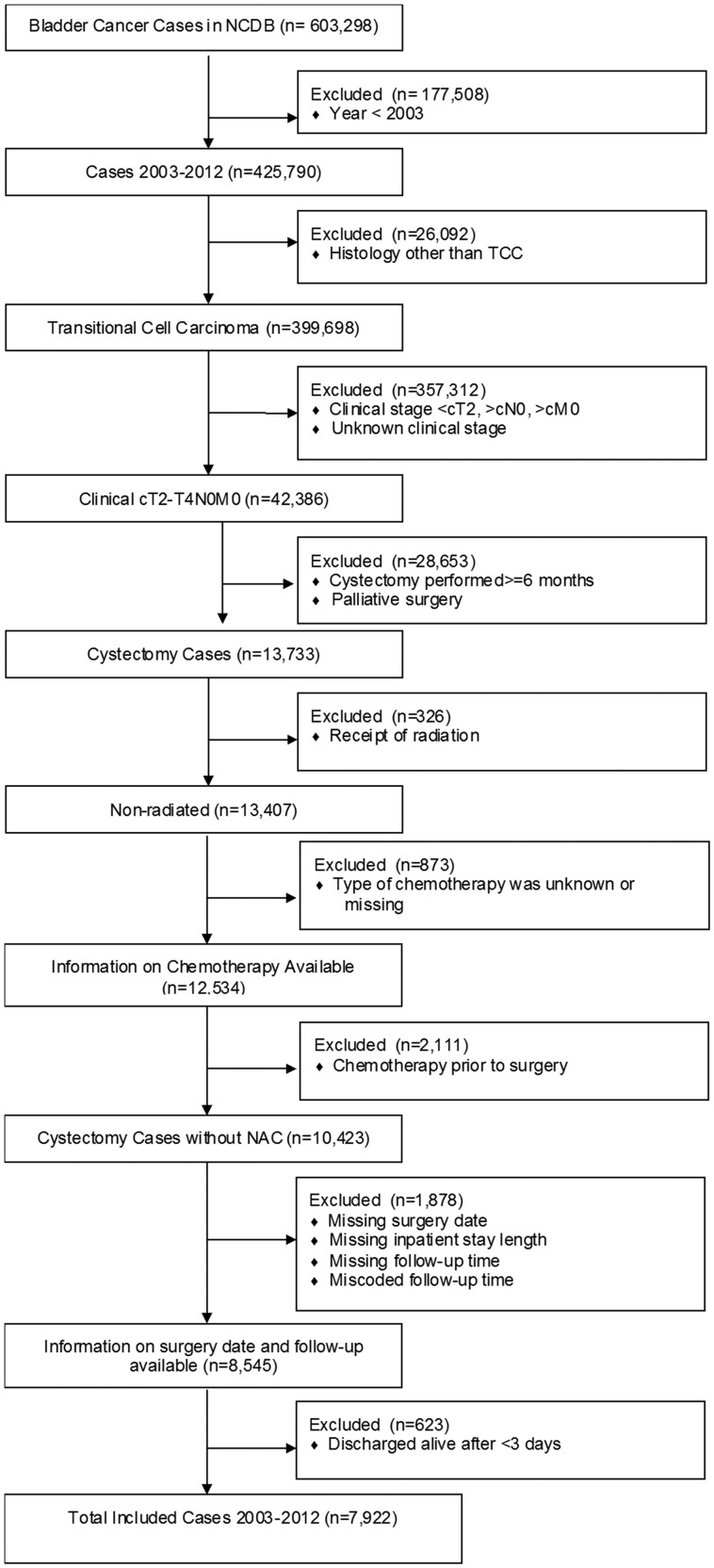
Methods: We identified patients with MIBC (cT2-T4aN0M0) who underwent RC without perioperative chemotherapy within the National Cancer Database (2003-2012). Using multistate multivariable modeling, we calculated time spent in three health states: hospitalized, discharged, and death more than 90 days postcystectomy. Cross-validation was performed by geographic region. Time spent in each state was weighted by utility to determine 90-day quality-adjusted life days (QALDs).
Results: Among 7922 patients, 90-day mortality was 7.6% (8.0% for lower and 6.7% for higher volume hospitals). Increasing age, clinical T stage, Charlson Comorbidity Index, and lower volume were associated with higher 90-day mortality and were included in the model. Cross-validation revealed appropriate performance (C-statistics of 0.53-0.74; calibration slopes of 0.50-1.67). The model predicted 25% of patients had a 90-day mortality risk higher than 10%, and observed 90-day mortality in this group was 14.0% (95% CI = 12.5% to 15.6%). Mean quality-adjusted life days (QALDs) was 63 (range = 44-68).
Conclusions: RC is associated with relatively high early mortality risk. Pretreatment variables may identify patients at particularly high risk, which may inform clinical trial design, facilitate shared decision making, and enhance quality improvement initiatives.
Figures




References
-
- Clark PE, Agarwal N, Biagioli MC et al. . Bladder cancer. J Natl Compr Canc Netw. 2013;114:446–475. - PubMed
-
- Boorjian SA, Kim SP, Tollefson MK et al. . Comparative performance of comorbidity indices for estimating perioperative and 5-year all cause mortality following radical cystectomy for bladder cancer. J Urol. 2013;1901:55–60. - PubMed
-
- Edwards BK, Howe HL, Ries LA et al. . Annual report to the nation on the status of cancer, 1973–1999, featuring implications of age and aging on U.S. cancer burden. Cancer. 2002;9410:2766–2792. - PubMed
-
- Gray PJ, Fedewa SA, Shipley WU et al. . Use of potentially curative therapies for muscle-invasive bladder cancer in the United States: results from the National Cancer Data Base. Eur Urol. 2013;635:823–829. - PubMed
-
- James ND, Hussain SA, Hall E et al. . Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer. N Engl J Med. 2012;36616:1477–1488. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources