

Long-term Outcomes of Stereotactic Body Radiotherapy for Low-Risk and Intermediate-Risk Prostate Cancer
- PMID: 30735235
- PMCID: PMC6484596
- DOI: 10.1001/jamanetworkopen.2018.8006
Long-term Outcomes of Stereotactic Body Radiotherapy for Low-Risk and Intermediate-Risk Prostate Cancer
Abstract
Importance: Stereotactic body radiotherapy harnesses improvements in technology to allow the completion of a course of external beam radiotherapy treatment for prostate cancer in the span of 4 to 5 treatment sessions. Although mounting short-term data support this approach, long-term outcomes have been sparsely reported.
Objective: To assess long-term outcomes after stereotactic body radiotherapy for low-risk and intermediate-risk prostate cancer.
Design, setting, and participants: This cohort study analyzed individual patient data from 2142 men enrolled in 10 single-institution phase 2 trials and 2 multi-institutional phase 2 trials of stereotactic body radiotherapy for low-risk and intermediate-risk prostate cancer between January 1, 2000, and December 31, 2012. Statistical analysis was performed based on follow-up from January 1, 2013, to May 1, 2018.
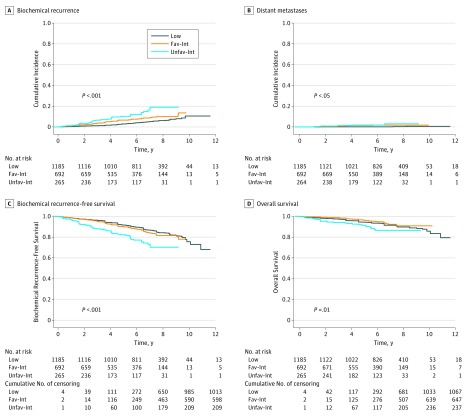
Main outcomes and measures: The cumulative incidence of biochemical recurrence was estimated using a competing risk framework. Physician-scored genitourinary and gastrointestinal toxic event outcomes were defined per each individual study, generally by Radiation Therapy Oncology Group or Common Terminology Criteria for Adverse Events scoring systems. After central review, cumulative incidences of late grade 3 or higher toxic events were estimated using a Kaplan-Meier method.
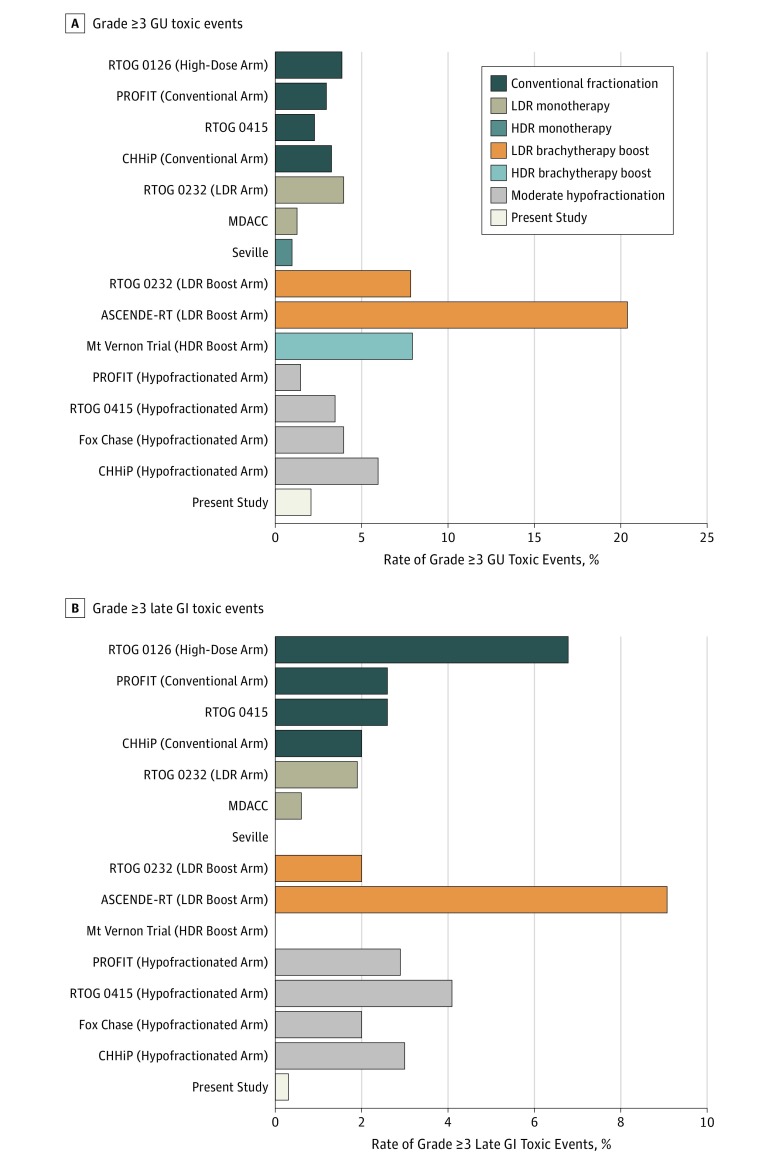
Results: A total of 2142 men (mean [SD] age, 67.9 [9.5] years) were eligible for analysis, of whom 1185 (55.3%) had low-risk disease, 692 (32.3%) had favorable intermediate-risk disease, and 265 (12.4%) had unfavorable intermediate-risk disease. The median follow-up period was 6.9 years (interquartile range, 4.9-8.1 years). Seven-year cumulative rates of biochemical recurrence were 4.5% (95% CI, 3.2%-5.8%) for low-risk disease, 8.6% (95% CI, 6.2%-11.0%) for favorable intermediate-risk disease, 14.9% (95% CI, 9.5%-20.2%) for unfavorable intermediate-risk disease, and 10.2% (95% CI, 8.0%-12.5%) for all intermediate-risk disease. The crude incidence of acute grade 3 or higher genitourinary toxic events was 0.60% (n = 13) and of gastrointestinal toxic events was 0.09% (n = 2), and the 7-year cumulative incidence of late grade 3 or higher genitourinary toxic events was 2.4% (95% CI, 1.8%-3.2%) and of late grade 3 or higher gastrointestinal toxic events was 0.4% (95% CI, 0.2%-0.8%).
Conclusions and relevance: In this study, stereotactic body radiotherapy for low-risk and intermediate-risk disease was associated with low rates of severe toxic events and high rates of biochemical control. These data suggest that stereotactic body radiotherapy is an appropriate definitive treatment modality for low-risk and intermediate-risk prostate cancer.
Conflict of interest statement
Figures
References
-
- National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: prostate cancer. Version I. https://www2.tri-kobe.org/nccn/guideline/urological/english/prostate.pdf. Accessed November 30, 2015.
-
- Dearnaley D, Syndikus I, Mossop H, et al. ; CHHiP Investigators . Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial. Lancet Oncol. 2016;17(8):1047-1060. doi: 10.1016/S1470-2045(16)30102-4 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
