

Prognostic Value of Vasodilator Stress Cardiac Magnetic Resonance Imaging: A Multicenter Study With 48 000 Patient-Years of Follow-up
- PMID: 30735566
- PMCID: PMC6439546
- DOI: 10.1001/jamacardio.2019.0035
Prognostic Value of Vasodilator Stress Cardiac Magnetic Resonance Imaging: A Multicenter Study With 48 000 Patient-Years of Follow-up
Erratum in
-
Error in Conflict of Interest Disclosure.JAMA Cardiol. 2019 May 1;4(5):497. doi: 10.1001/jamacardio.2019.0951. JAMA Cardiol. 2019. PMID: 30969317 Free PMC article. No abstract available.
Abstract
Importance: Stress cardiac magnetic resonance imaging (CMR) is not widely used in current clinical practice, and its ability to predict patient mortality is unknown.
Objective: To determine whether stress CMR is associated with patient mortality.
Design, setting, and participants: Real-world evidence from consecutive clinically ordered CMR examinations. Multicenter study of patients undergoing clinical evaluation of myocardial ischemia. Patients with known or suspected coronary artery disease (CAD) underwent clinical vasodilator stress CMR at 7 different hospitals. An automated process collected data from the finalized clinical reports, deidentified and aggregated the data, and assessed mortality using the US Social Security Death Index.
Main outcomes and measures: All-cause patient mortality.
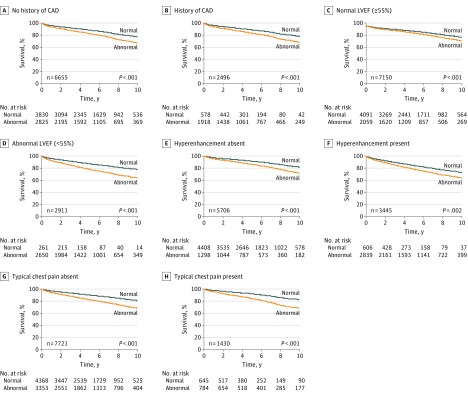
Results: Of the 9151 patients, the median (interquartile range) patient age was 63 (51-70) years, 55% were men, and the median (interquartile range) body mass index was 29 (25-33) (calculated as weight in kilograms divided by height in meters squared). The multicenter automated process yielded 9151 consecutive patients undergoing stress CMR, with 48 615 patient-years of follow-up. Of these patients, 4408 had a normal stress CMR examination, 4743 had an abnormal examination, and 1517 died during a median follow-up time of 5.0 years. Using multivariable analysis, addition of stress CMR improved prediction of mortality in 2 different risk models (model 1 hazard ratio [HR], 1.83; 95% CI, 1.63-2.06; P < .001; model 2: HR, 1.80; 95% CI, 1.60-2.03; P < .001) and also improved risk reclassification (net improvement: 11.4%; 95% CI, 7.3-13.6; P < .001). After adjustment for patient age, sex, and cardiac risk factors, Kaplan-Meier survival analysis showed a strong association between an abnormal stress CMR and mortality in all patients (HR, 1.883; 95% CI, 1.680-2.112; P < .001), patients with (HR, 1.955; 95% CI, 1.712-2.233; P < .001) and without (HR, 1.578; 95% CI, 1.235-2.2018; P < .001) a history of CAD, and patients with normal (HR, 1.385; 95% CI, 1.194-1.606; P < .001) and abnormal left ventricular ejection fraction (HR, 1.836; 95% CI, 1.299-2.594; P < .001).
Conclusions and relevance: Clinical vasodilator stress CMR is associated with patient mortality in a large, diverse population of patients with known or suspected CAD as well as in multiple subpopulations defined by history of CAD and left ventricular ejection fraction. These findings provide a foundational motivation to study the comparative effectiveness of stress CMR against other modalities.
Conflict of interest statement
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
