

Are we mis-estimating chemotherapy-induced peripheral neuropathy? Analysis of assessment methodologies from a prospective, multinational, longitudinal cohort study of patients receiving neurotoxic chemotherapy
- PMID: 30736741
- PMCID: PMC6368751
- DOI: 10.1186/s12885-019-5302-4
Are we mis-estimating chemotherapy-induced peripheral neuropathy? Analysis of assessment methodologies from a prospective, multinational, longitudinal cohort study of patients receiving neurotoxic chemotherapy
Abstract
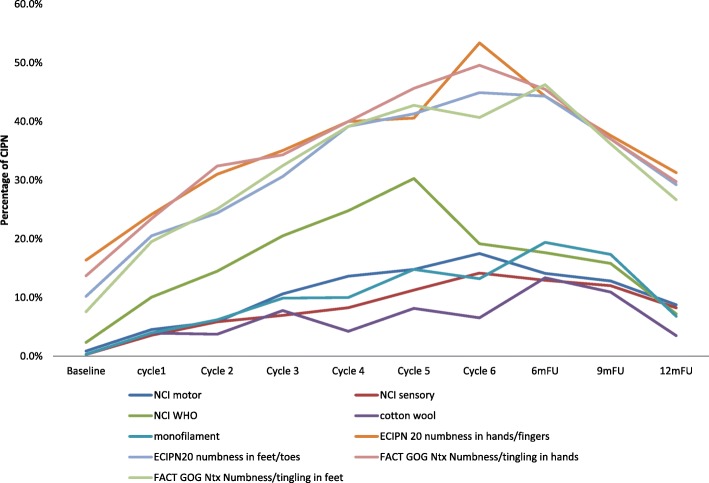
Background: There are inconsistencies in the literature regarding the prevalence and assessment of chemotherapy-induced peripheral neuropathy (CIPN). This study explored CIPN natural history and its characteristics in patients receiving taxane- and platinum-based chemotherapy.
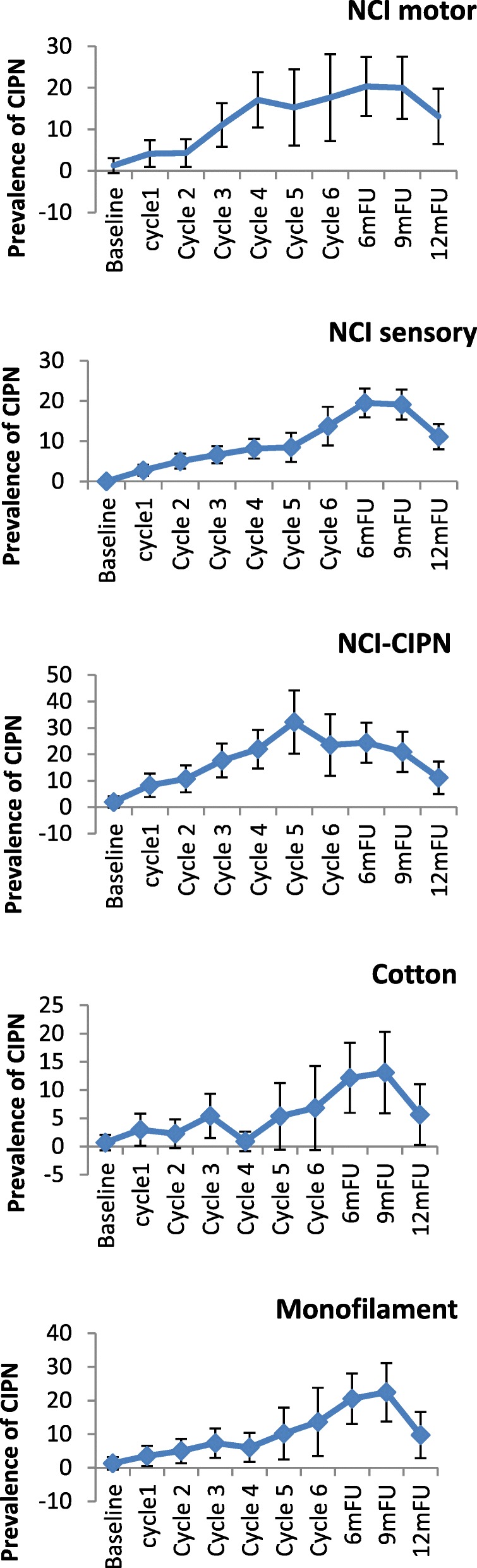
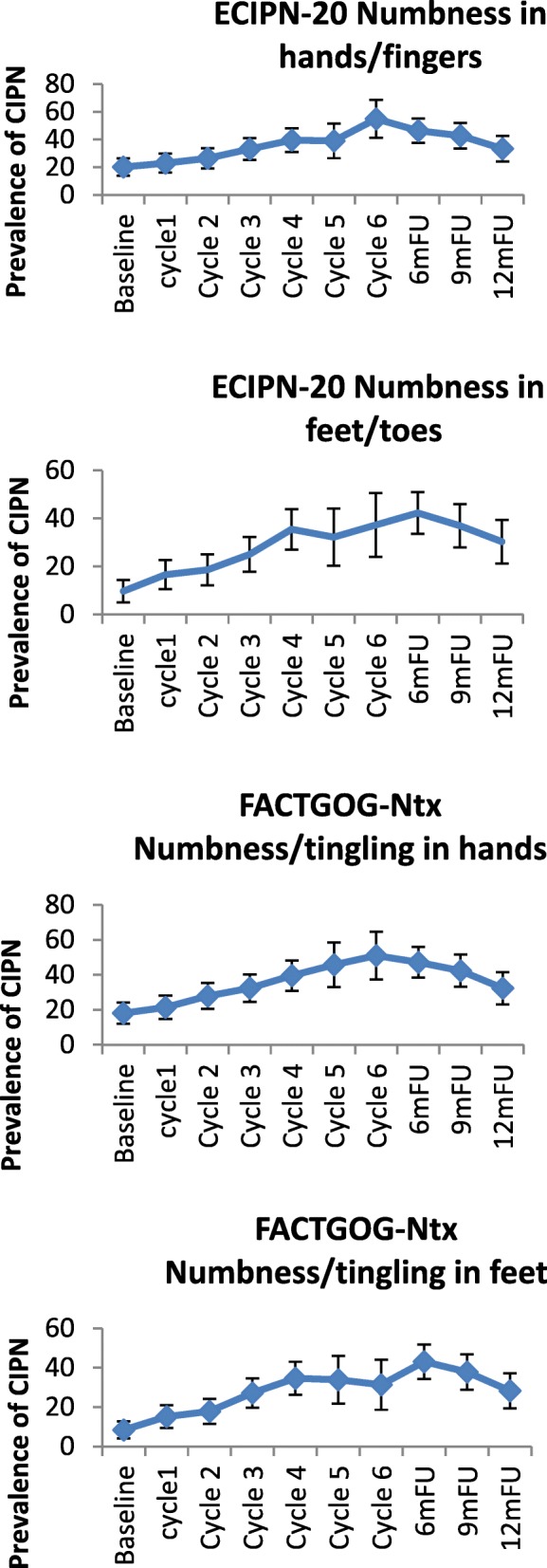
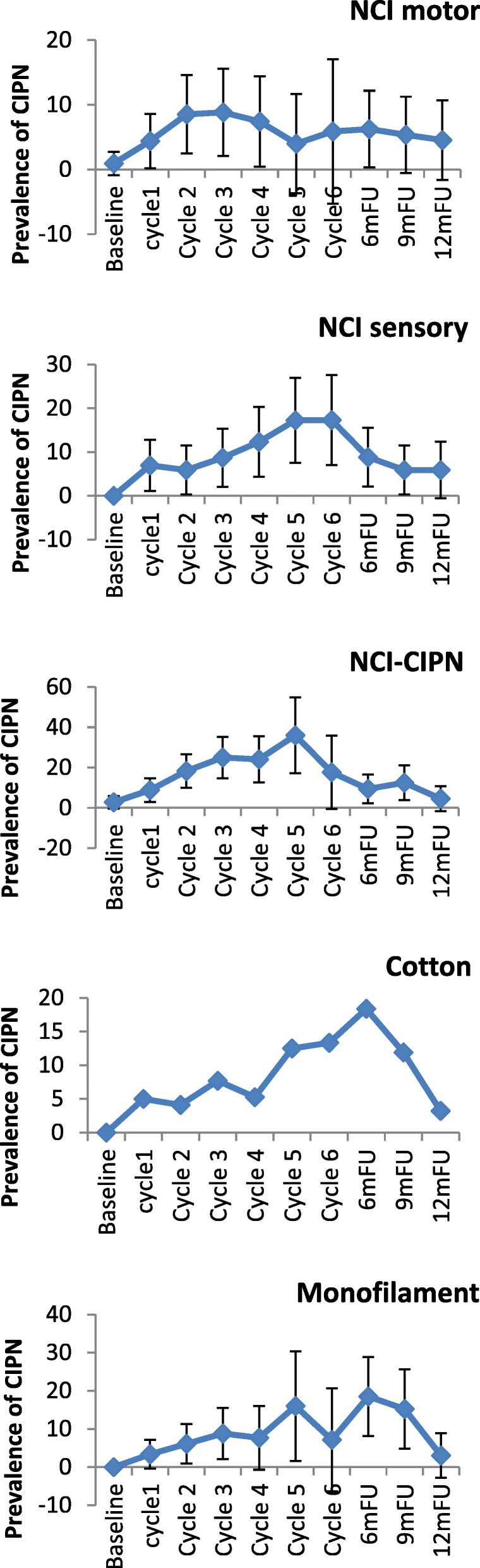
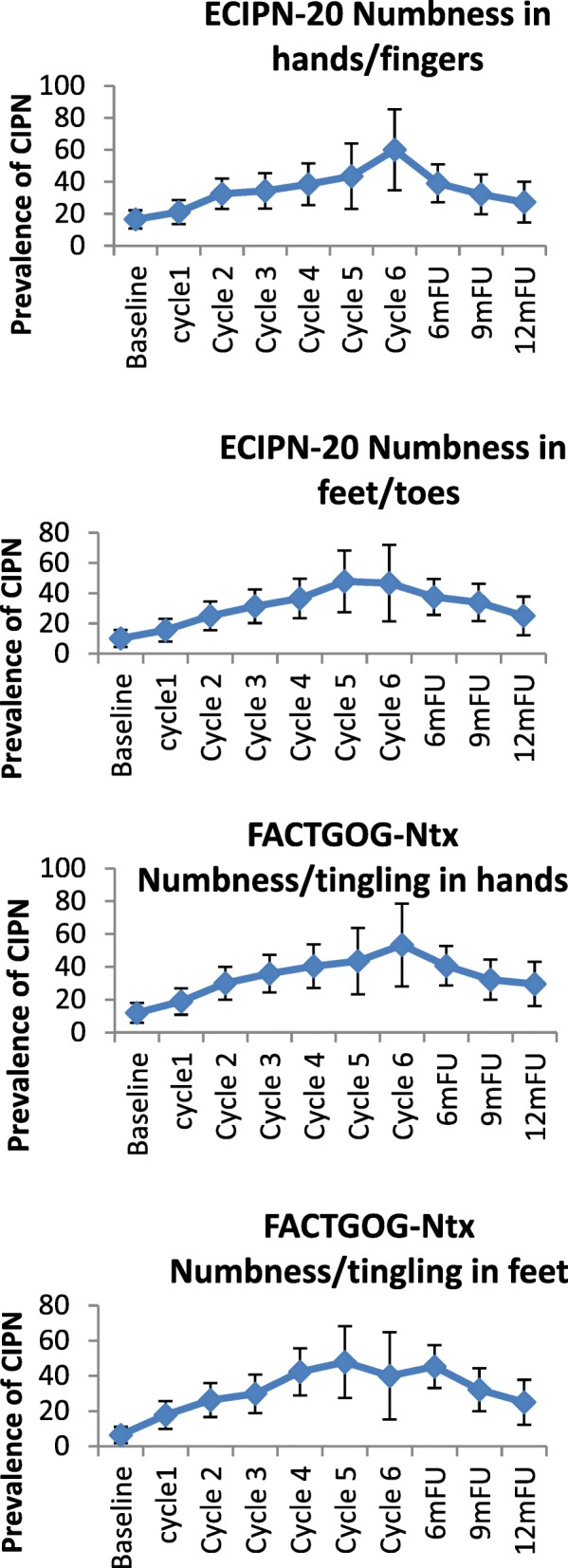
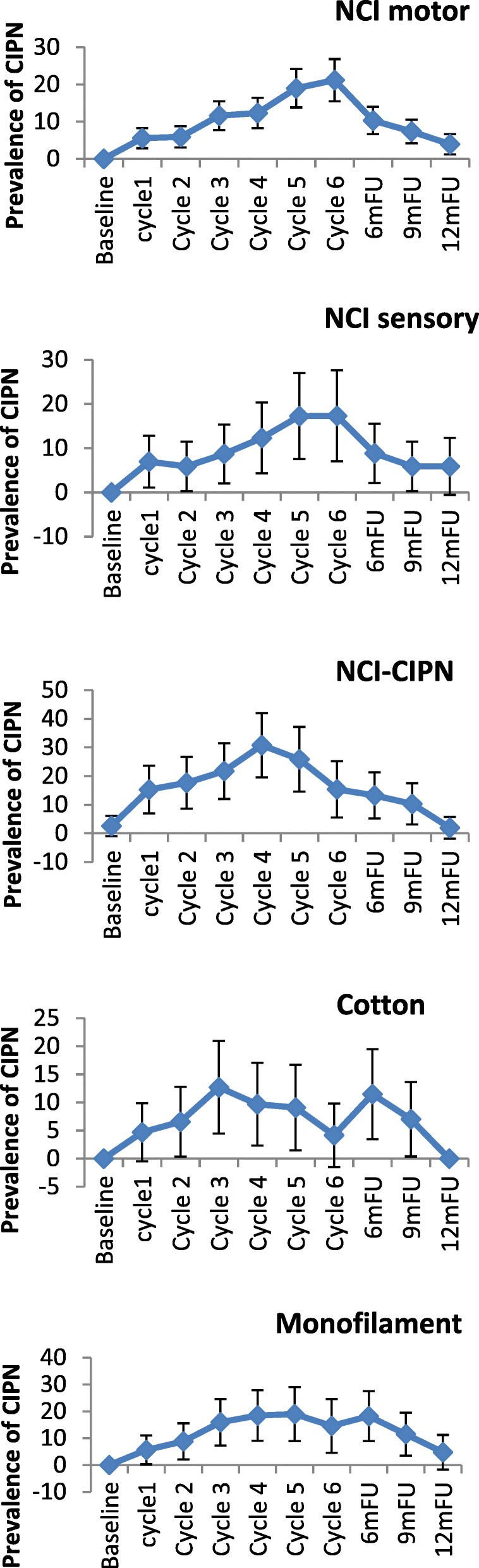
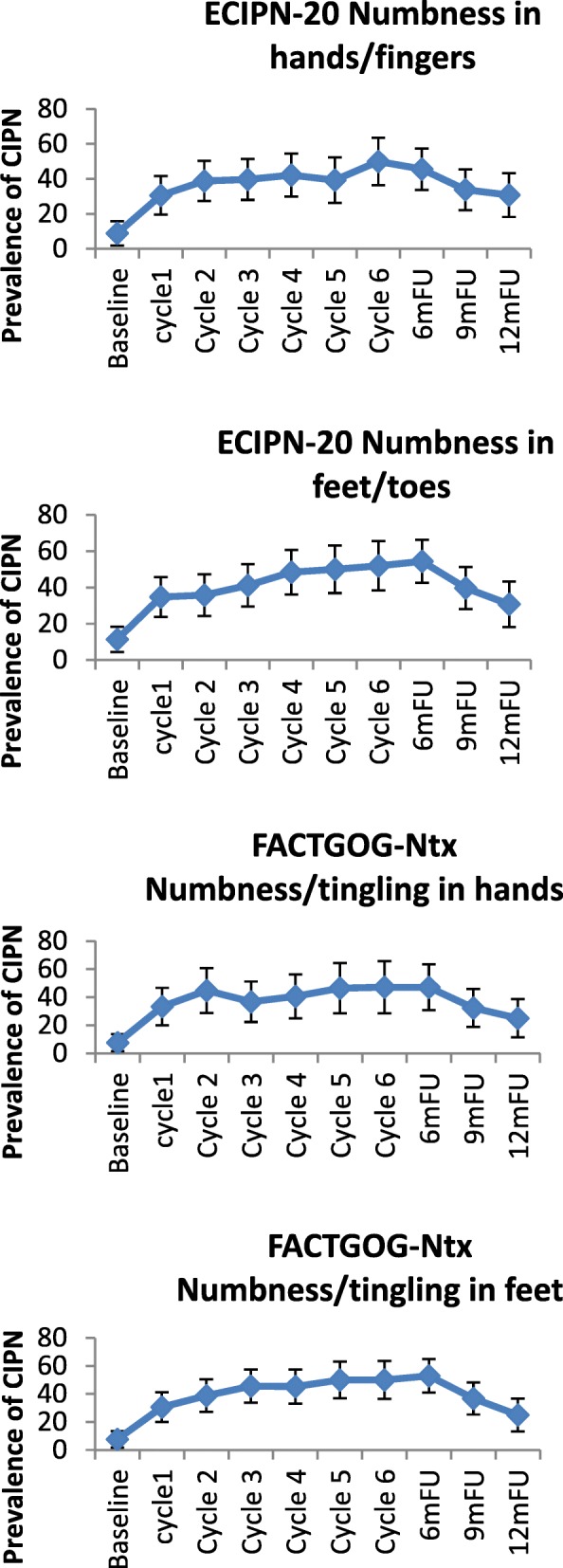
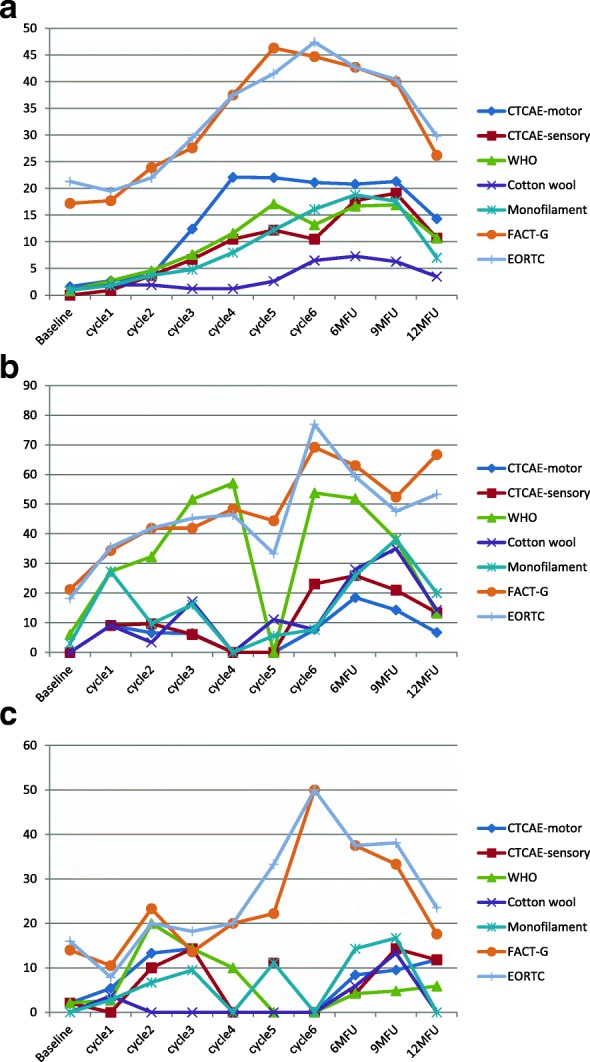
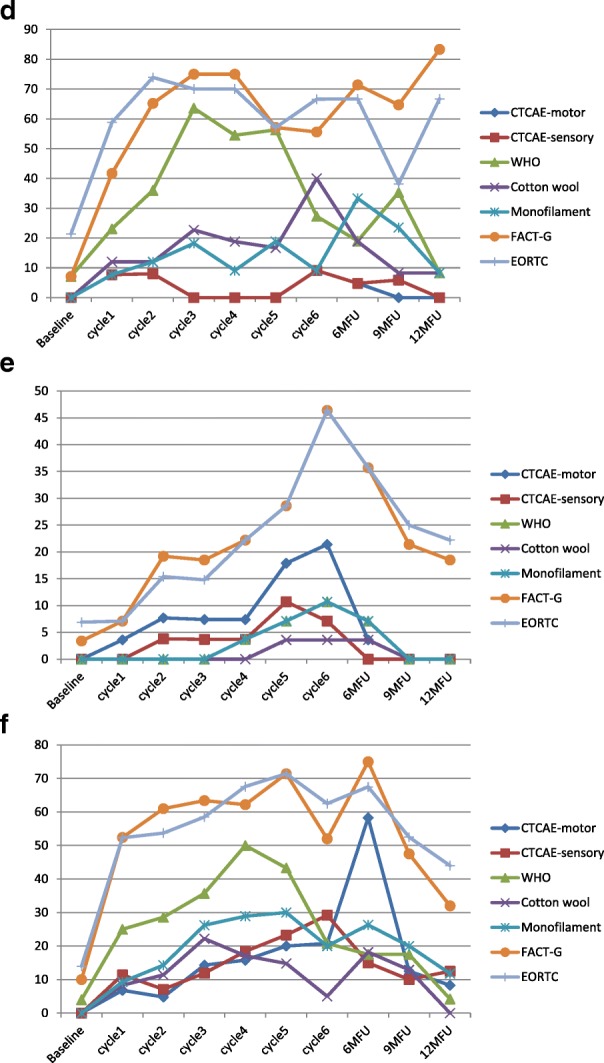
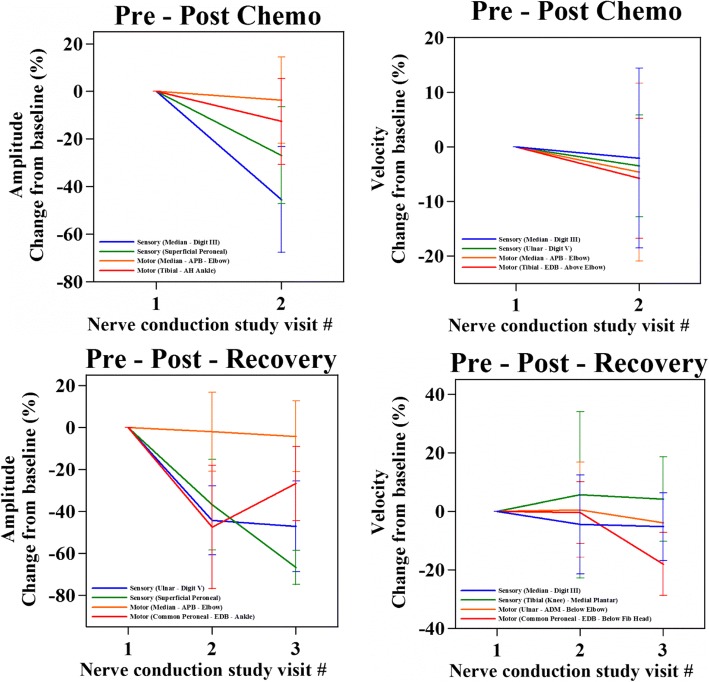
Patients and methods: Multi-country multisite prospective longitudinal observational study. Patients were assessed before commencing and three weekly during chemotherapy for up to six cycles, and at 6,9, and 12 months using clinician-based scales (NCI-CTCAE; WHO-CIPN criterion), objective assessments (cotton wool test;10 g monofilament); patient-reported outcome measures (FACT/GOG-Ntx; EORTC-CIPN20), and Nerve Conduction Studies.
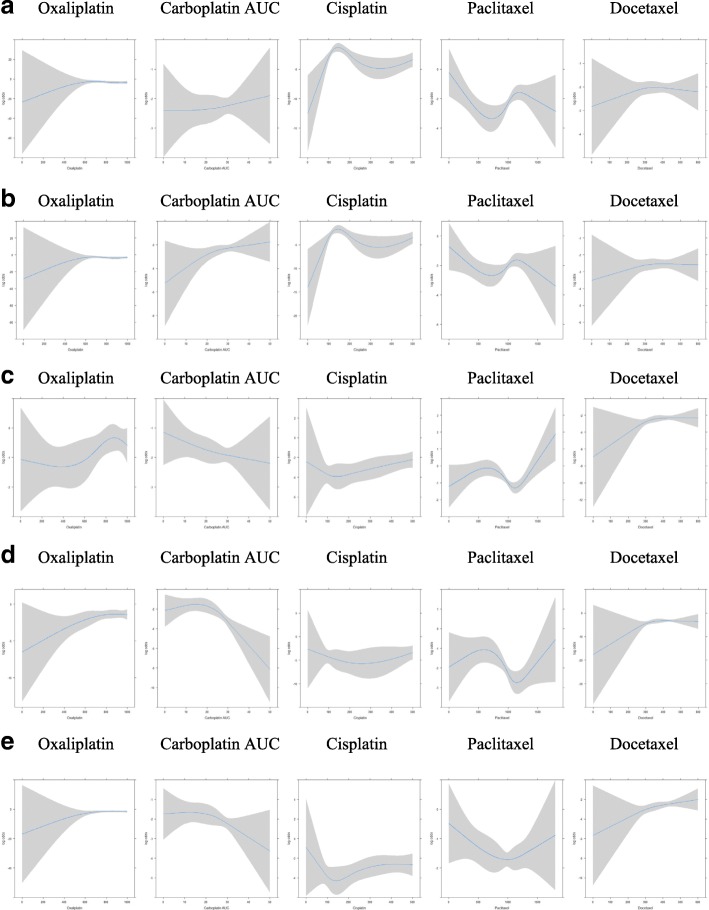
Results: In total, 343 patients were recruited in the cohort, providing 2399 observations. There was wide variation in CIPN prevalence rates using different assessments (14.2-53.4%). Prevalence of sensory neuropathy (and associated symptom profile) was also different in each type of chemotherapy, with paclitaxel (up to 63%) and oxaliplatin (up to 71.4%) showing the highest CIPN rates in most assessments and a more complex symptom profile. Peak prevalence was around the 6-month assessment (up to 71.4%). Motor neurotoxicity was common, particularly in the docetaxel subgroup (up to 22.1%; detected by NCI-CTCAE). There were relatively moderately-to-low correlations between scales (rs = 0.15,p < 0.05-rs = 0.48 p < 0.001), suggesting that they measure different neurotoxicity aspects from each other. Cumulative chemotherapy dose was not associated with onset and course of CIPN.
Conclusion: The historical variation reported in CIPN incidence and prevalence is possibly confounded by disagreement between assessment modalities. Clinical practice should consider assessment of motor neuropathy for neurotoxic chemotherapy. Current scales may not be all appropriate to measure CIPN in a valid way, and a combination of scales are needed.
Keywords: Assessment; Cancer; Chemotherapy; Neurotoxicity; Peripheral neuropathy; Platins; Taxanes.
Conflict of interest statement
Ethics approval and consent to participate
The study has been approved by the ethics committees of the Hong Kong Polytechnic University, Hong Kong; Central Cluster of the Hospital Authority, Hong Kong; The National University Hospital; Singapore; The University of Manchester, Manchester, UK; and the Central Manchester Research and Ethics Committee. All participants have provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Miaskowski C, Mastick J, Paul SM, Topp K, Smoot B, Abrams G, Chen LM, Kober KM, Conley YP, Chesney M, Bolla K, Mausisa G, Mazor M, Wong M, Schumacher M, Levine JD. Chemotherapy-induced neuropathy in Cancer survivors. J Pain Symptom Manag. 2017;54(2):204–218. doi: 10.1016/j.jpainsymman.2016.12.342. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
