

Comparing Australian orthopaedic surgeons' reported use of thromboprophylaxis following arthroplasty in 2012 and 2017
- PMID: 30736774
- PMCID: PMC6368726
- DOI: 10.1186/s12891-019-2409-3
Comparing Australian orthopaedic surgeons' reported use of thromboprophylaxis following arthroplasty in 2012 and 2017
Abstract
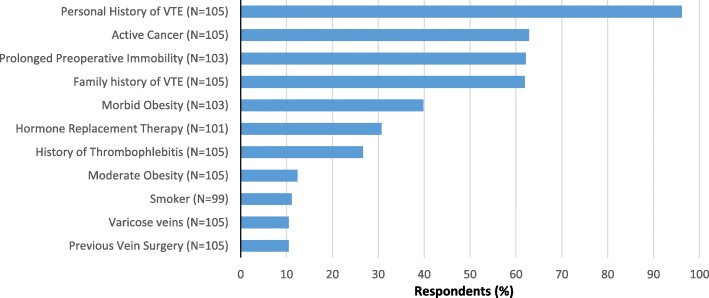
Background: It is generally accepted that all arthroplasty patients should receive venous thromboembolism (VTE) and bleeding risk assessments, and that postoperative thromboprophylaxis be routinely prescribed where appropriate. Guideline recommendations regarding what to prescribe, however, have been inconsistent over the years, particularly regarding the appropriateness of aspirin. Our aim was to explore thromboprophylaxis patterns in use following hip and knee arthroplasty in Australia, and to examine associated variables.
Methods: Orthopaedic surgeons were invited via mail to participate in two national surveys, conducted in 2012 (N = 478) and 2017 (N = 820), respectively.
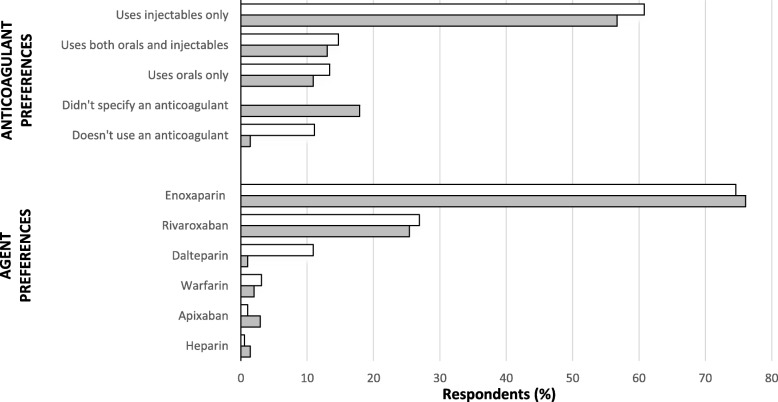
Results: The final response rates were 50.0 and 65.8% for 2012 and 2017, respectively. The thromboprophylaxis prescribing routines reported by respondents were divided into four categories: anticoagulant-only (the same anticoagulant-only routine for everyone), aspirin-only (aspirin for everyone), staged-supply (an anticoagulant during the initial postoperative period, followed by aspirin, for everyone) and risk-stratification routines (differing regimens depending on patients' perceived risk of VTE). The most common approaches reported were anticoagulant-only routines; however, their popularity almost halved within the five-year period (from ~ 74% to ~ 41%). Conversely, staged-supply and risk-stratification protocol usage increased by more than two and nine times, respectively. In 2017, over one-half of surgeons reported prescribing aspirin in their practice. Reported concern for postoperative VTE and infections (OR 0.555 95% CI 0.396-0.779, p = 0.001 and OR 1.455 95% CI 1.010-2.097, p = 0.044 respectively), as well as Arthroplasty Society membership (OR 2.814 95% CI 1.367-5.790, p = 0.005) were predictors for use of aspirin (Cox and Snell R square = 0.072). The factor most commonly reported to shape surgeons' protocols was research literature. Factors limiting prescribing of pharmacological prophylaxis included a perception that it increases bleeding and wound infection risk, is inconvenient, and lacks evidence applicable to real-world practice.
Conclusions: VTE prevention post-arthroplasty is an evolving and multi-faceted entity, influenced by a range of factors and seemingly in need of robust evidence from large clinical trials to guide practice. The data highlighted potential short-falls in practice related to aspirin over-use, which could be further explored and addressed in future studies in order to optimise patient outcomes and reduce the significant morbidity and healthcare costs associated with VTE following these increasingly common surgical procedures.
Keywords: Arthroplasty; Aspirin; Guideline; Survey; Thromboprophylaxis; Venous thromboembolism.
Conflict of interest statement
Ethics approval and consent to participate
The two surveys were conducted as separate studies, each receiving ethics approval from the Tasmanian Social Science Human Research Ethics Committee (approval numbers: H001265 and H0016454, respectively). Consent was obtained by way of inference after participants read the information in their invitation letter, and then completed and returning the survey by post.
Consent for publication
This manuscript does not contain any individual surgeon’s data in any form (i.e.
Competing interests
CM and GP report declare no conflicts of interest. LB has received consultancy funding from Aspen Pharmacare Australia for the development of education materials related to warfarin therapy. LB has also received consultancy funding from Boehringer Ingelheim Pty Ltd. for the development of educational materials for dabigatran/atrial fibrillation and provision of expert advice regarding the optimal use of anticoagulants in the prevention of stroke.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
 Study 1;
Study 1;  Study 2
Study 2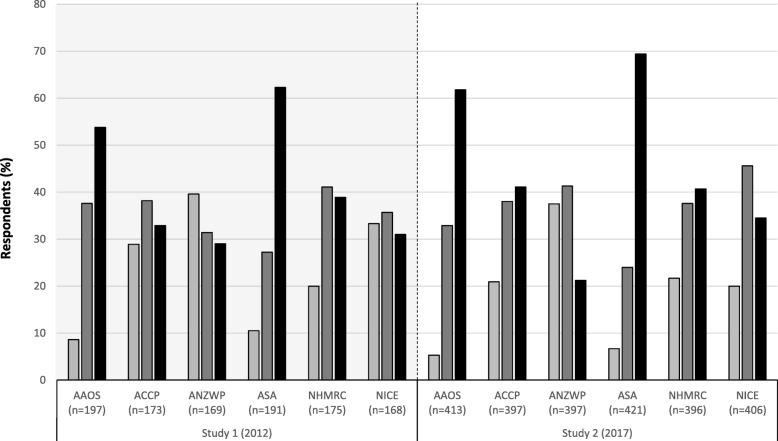
 Not come across before;
Not come across before;  Heard of in passing;
Heard of in passing;  Very familiar with
Very familiar with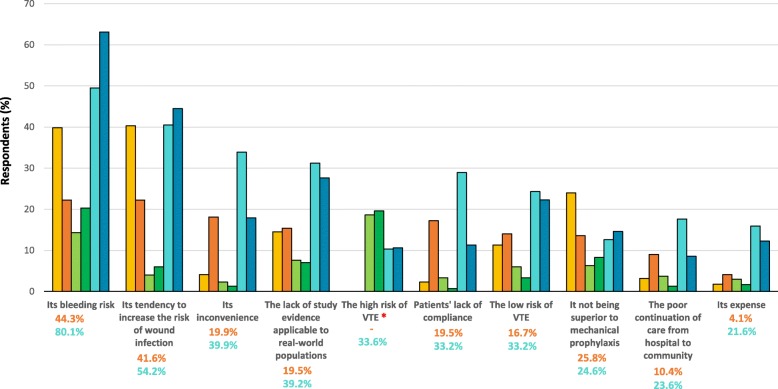
 Inpatient and
Inpatient and  Discharge pharmacological prophylaxis use (Study 1);
Discharge pharmacological prophylaxis use (Study 1);  Inpatient and
Inpatient and  Discharge aspirin use (Study 2); Inpatient
Discharge aspirin use (Study 2); Inpatient  and
and  Discharge anticoagulant use (Study 2). Total proportion of surgeons who answered the question in
Discharge anticoagulant use (Study 2). Total proportion of surgeons who answered the question in  and
and 
 Pharmacological prophylaxis (Study 1); Aspirin and Anticoagulant prophylaxis (Study 2)
Pharmacological prophylaxis (Study 1); Aspirin and Anticoagulant prophylaxis (Study 2)References
-
- Australian Orthopaedic Association. National Joint Replacement Registry: Reported Hip Procedures. https://aoanjrr.sahmri.com/hips. Accessed 20 May 2018.
-
- Australian Orthopaedic Association. National Joint Replacement Registry: Reported Knee Procedures. https://aoanjrr.sahmri.com/knees. Accessed 20 May 2018.
-
- National Joint Registry (UK). 14th Annual Report. Hertfordshire: National Joint Registry for England, Wales, Northern Ireland and the Isle of Man; 2017.
-
- Centers for Disease Control and Prevention (National Center for Health Statistics). Hospitalization for Total Hip Replacement Among Inpatients Aged 45 and Over: United States 2000–2010 2015. https://www.cdc.gov/nchs/products/databriefs/db186.htm. Accessed 20 May 2018.
-
- Centers for Disease Control and Prevention (National Center for Health Statistics). Hospitalization for Total Knee Replacement Among Inpatients Aged 45 and Over: United States 2000–2010 2015. https://www.cdc.gov/nchs/products/databriefs/db210.htm. Accessed 20 May 2018.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
