

New risk score for predicting progression of membranous nephropathy
- PMID: 30736804
- PMCID: PMC6368730
- DOI: 10.1186/s12967-019-1792-8
New risk score for predicting progression of membranous nephropathy
Abstract
Background: Patients with Idiopathic membranous nephropathy (IMN) have various outcomes. The aim of this study is to construct a tool for clinicians to precisely predict outcome of IMN.
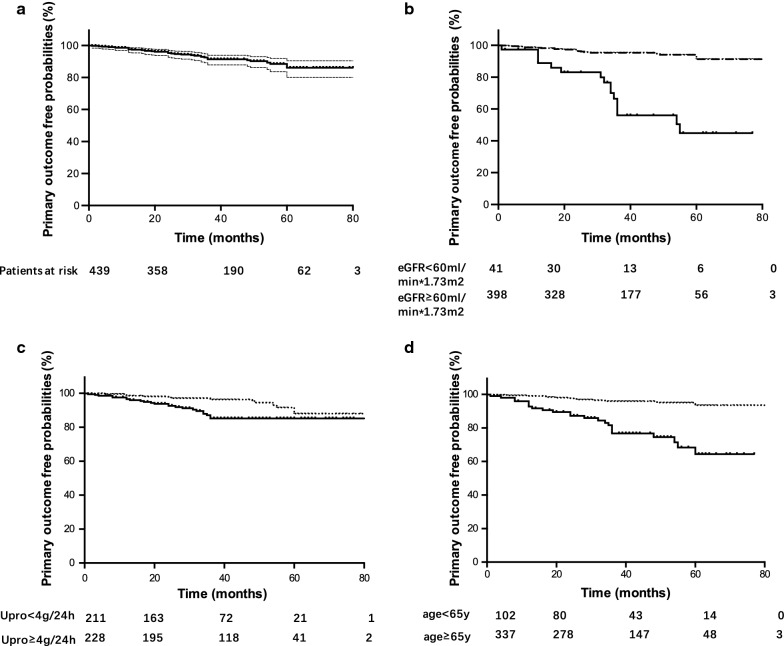
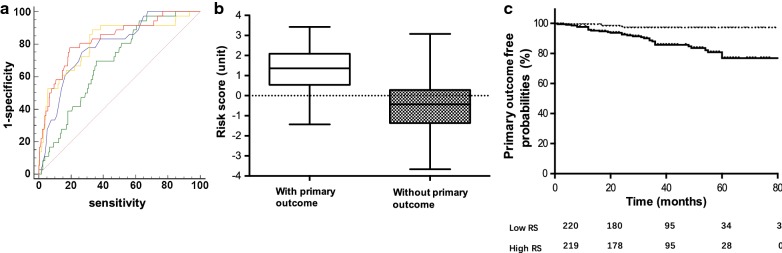
Methods: IMN patients diagnosed by renal biopsy from Shanghai Ruijin Hospital from 2009.01 to 2013.12 were enrolled in this study. Primary outcome was defined as a combination of renal function progression [defined as a reduction of estimated glomerular filtration rate (eGFR) equal to or over 30% comparing to baseline], ESRD or death. Risk models were established by Cox proportional hazard regression analysis and validated by bootstrap resampling analysis. ROC curve was applied to test the performance of risk score.
Results: Totally 439 patients were recruited in this study. The median follow-up time was 38.73 ± 19.35 months. The enrolled patients were 56 (15-83) years old with a male predominance (sex ratio: male vs female, 1:0.91). The median baseline serum albumin, eGFR-EPI and proteinuria were 23(8-43) g/l, 100.31(12.81-155.98) ml/min/1.73 m2 and 3.98(1.50-22.98) g/24 h, respectively. In total, there were 36 primary outcomes occurred. By Cox regression analysis, the best risk model included age [HR: 1.04(1.003-1.08), 95% CI from bootstrapping: 1.01-1.08), eGFR [HR: 0.97 (0.96-0.99), 95% CI from bootstrapping: 0.96-0.99) and proteinuria [HR: 1.09 (1.01-1.18), 95% CI from bootstrapping: 1.02-1.16). One unit increasing of the risk score based on the best model was associated with 2.57 (1.97-3.36) fold increased risk of combined outcome. The discrimination of this risk score was excellent in predicting combined outcome [C statistics: 0.83, 95% CI 0.76-0.90].
Conclusions: Our study indicated that older IMN patients with lower eGFR and heavier proteinuria at the time of renal biopsy were at a higher risk for adverse outcomes. A risk score based on these three variables provides clinicians with an effective tool for risk stratification.
Keywords: Chronic kidney disease; Membranous nephropathy; Prognosis; Risk score.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
