

Are tumor size changes predictive of survival for checkpoint blockade based immunotherapy in metastatic melanoma?
- PMID: 30736858
- PMCID: PMC6368769
- DOI: 10.1186/s40425-019-0513-4
Are tumor size changes predictive of survival for checkpoint blockade based immunotherapy in metastatic melanoma?
Abstract
Background: In oncology clinical development, objective response rate, disease control rate and early tumor size changes are commonly used as efficacy metrics for early decision-making. However, for immunotherapy trials, it is unclear whether these early efficacy metrics are still predictive of long-term clinical benefit such as overall survival. The goal of this paper is to identify appropriate early efficacy metrics predictive of overall survival for immunotherapy trials.
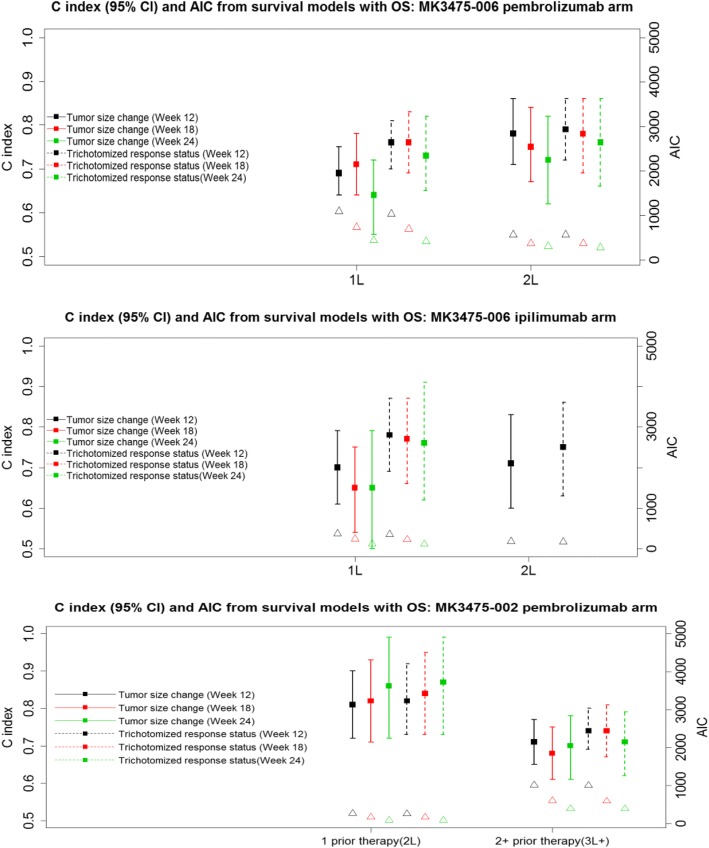
Methods: Based on several checkpoint blockade based immunotherapy studies in metastatic melanoma, we evaluated the predictive value of early tumor size changes and RECIST-based efficacy metrics at various time points on overall survival. The cut-off values for tumor size changes to predict survival were explored via tree based recursive partitioning and validated by external data. Sensitivity analyses were performed for the cut-offs.
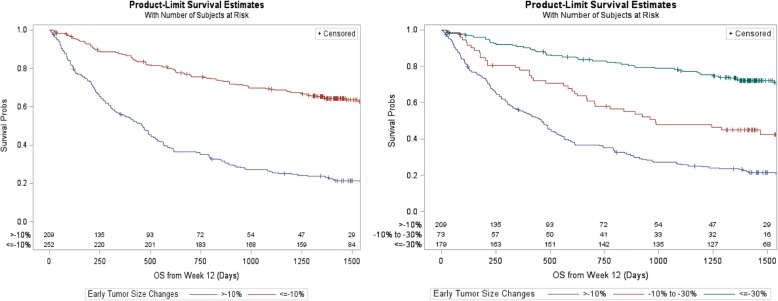
Results: The continuous tumor size change metric and RECIST-based trichotomized response metric at different landmark time points were found to be statistically significantly associated with overall survival. The predictive values were higher at Week 12 and 18 than those at Week 24. The percentage of tumor size changes appeared to have comparable or lower predictive values than the RECIST-based trichotomized metric, and a cut-off of approximately 10% tumor reduction appeared to be reasonable for predicting survival.
Conclusions: An approximate 10% tumor reduction may be a reasonable cut-off for early decision-making while the RECIST-based efficacy metric remains the primary tool. Early landmark analysis is especially useful for decision making when accrual is fast. Composite response rate (utilizing different weights for PR/CR and SD) may be worth further investigation.
Trial registration: Clinical trials gov, NCT01295827 , Registered February 15, 2011; NCT01704287 , Registered October 11, 2012; NCT01866319 , Registered May 31, 2013.
Keywords: Cut-off values; Early efficacy metrics; Early tumor size changes; Immunotherapy trials; RECIST.
Conflict of interest statement
Ethics approval and consent to participate
All three study protocols and amendments were approved by appropriate institutional review boards and ethics committees at each institution. The studies were done in accordance with the protocols, Good Clinical Practice guidelines, and the declaration of Helsinki. All patients provided written informed consent. The studies were registered on
Consent for publication
Not applicable.
Competing interests
MW, CC, TJ, JA, NL, PK, NI and SE are employed by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA, and hold stock in the company. CH serves as a research consultant for Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Eisenhauer E, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R., et al.. New response evaluation criteria in solid tumors: revised RECIST guideline (version 1.1). Eur J Cancer, 2009;45(2):228–247. - PubMed
-
- Karrison TG, Maitland ML, Stadler WM, Ratain MJ. Design of Phase II Cancer trials using a continuous endpoint of change in tumor size: application to a study of Sorafenib and Erlotinib in non–small-cell NSCLC Cancer. J Natl Cancer Inst. 2007;99(19):1455–1461. doi: 10.1093/jnci/djm158. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials