

Macrophages in Heart Failure with Reduced versus Preserved Ejection Fraction
- PMID: 30737012
- PMCID: PMC6552663
- DOI: 10.1016/j.molmed.2019.01.002
Macrophages in Heart Failure with Reduced versus Preserved Ejection Fraction
Abstract
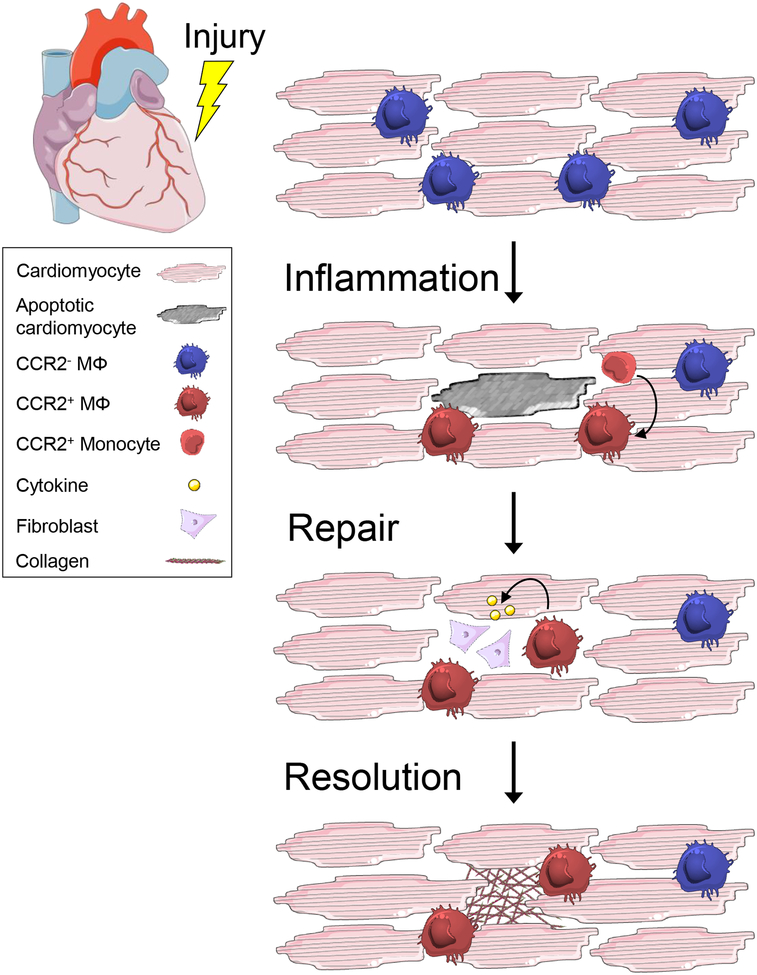
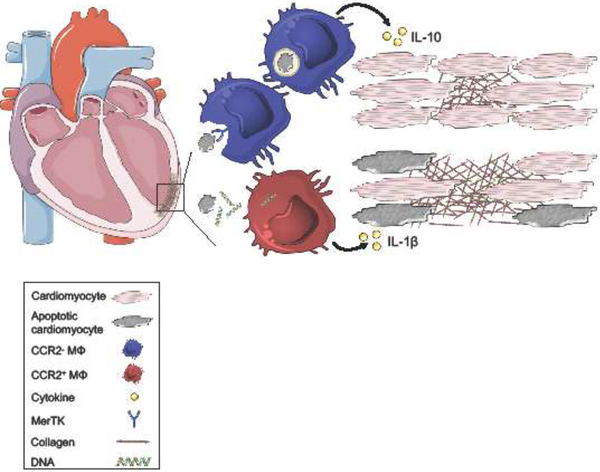
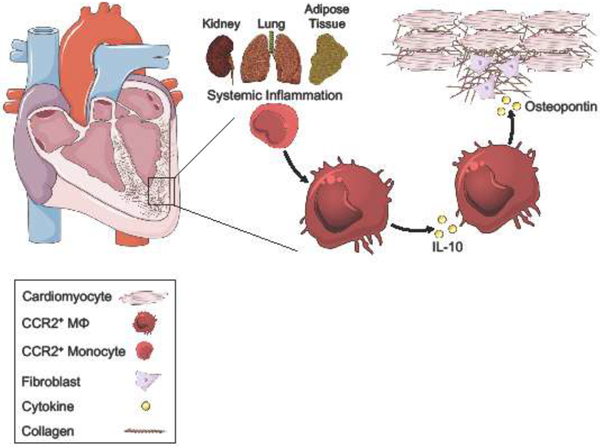
There is a growing number of individuals living with heart failure (HF) with reduced ejection fraction (HFrEF) or preserved ejection fraction (HFpEF). Long-term prognosis remains poor in both cases, especially in HFpEF, which is rising in incidence and lacks effective therapeutics. In both HFrEF and HFpEF, there is evidence that elevated inflammatory biomarkers, implicating innate immune cells such as macrophages, are associated with worsened clinical outcomes. Macrophage subsets are active in both inflammatory and reparative processes, yet our understanding of the causative roles for these cells in HF development and progression is incomplete. Here, we discuss recent findings interrogating the role of macrophages in inflammation and its resolution in the context of HF, with a specific focus on HFrEF versus HFpEF.
Keywords: heart failure; inflammation; macrophage; preserved ejection fraction; reduced ejection fraction.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Figures
References
-
- Benjamin EJ et al. (2018) Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 137 (12), e67–e492. - PubMed
-
- Yancy CW et al. (2017) 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Card Fail 23 (8), 628–651. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
