

Kinesiologic considerations for targeting activation of scapulothoracic muscles - part 1: serratus anterior
- PMID: 30737019
- PMCID: PMC6849091
- DOI: 10.1016/j.bjpt.2019.01.008
Kinesiologic considerations for targeting activation of scapulothoracic muscles - part 1: serratus anterior
Abstract
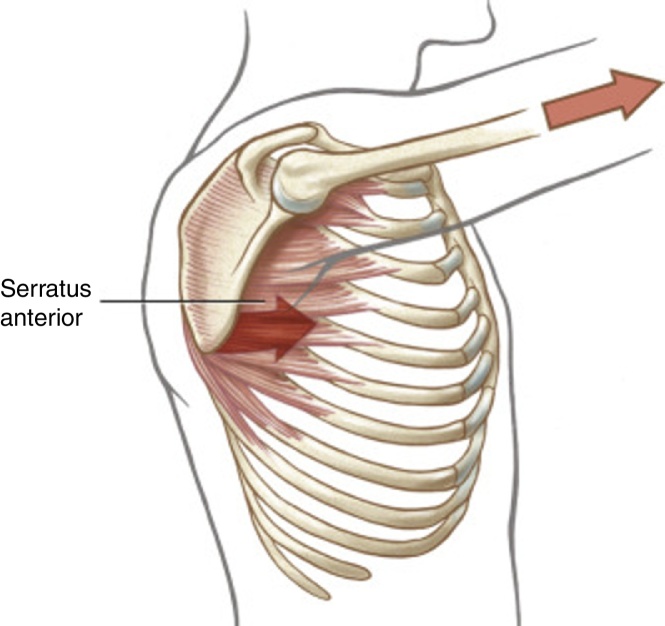
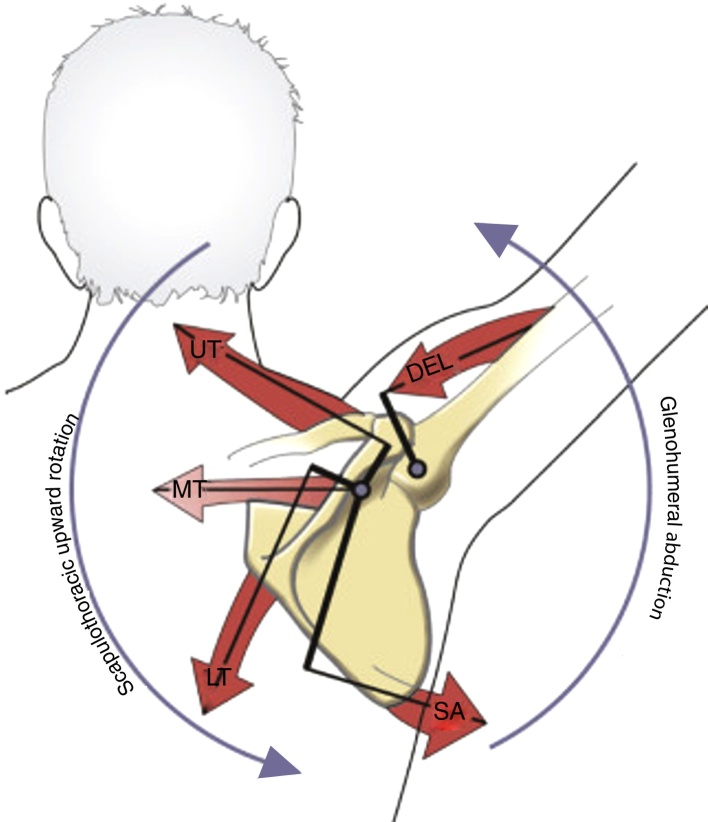
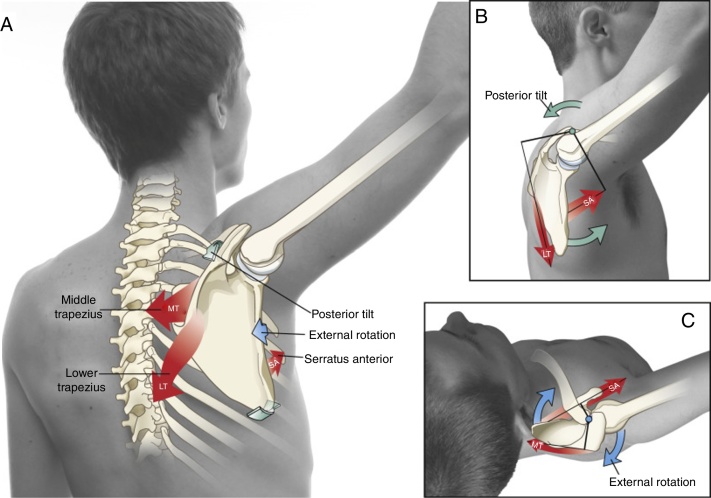
Background: The serratus anterior (SA) is capable of a wide range of actions across the scapulothoracic joint. Furthermore, the lack of control, strength, or activation of this important muscle is believed to be associated with several painful conditions involving the shoulder complex. Studies and clinical intuition have therefore identified several exercises that selectively target the activation of the SA.
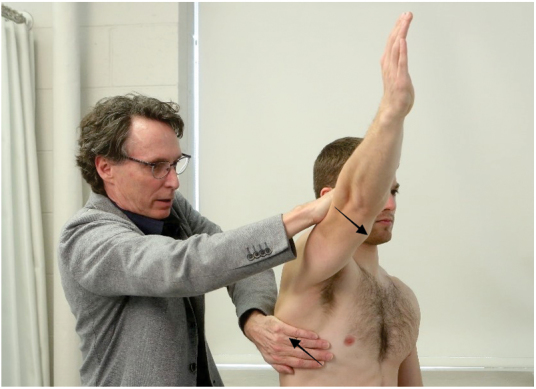
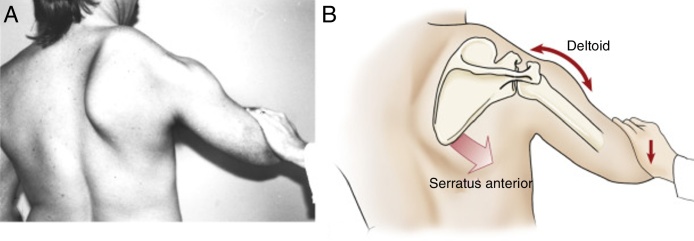
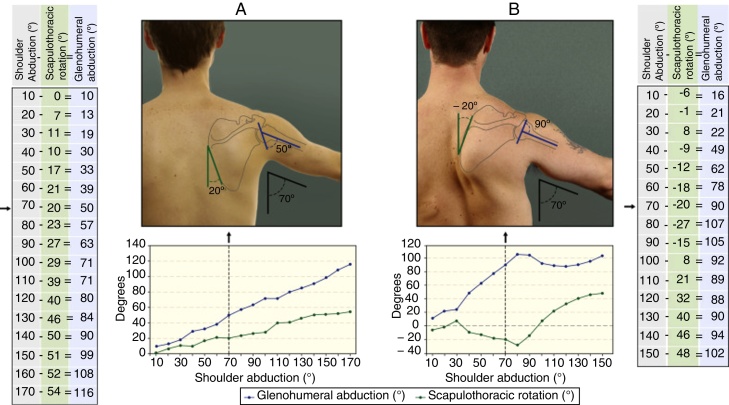
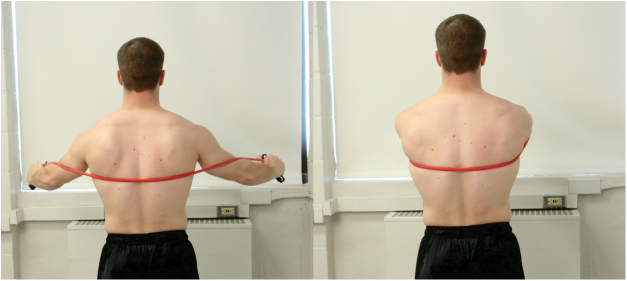
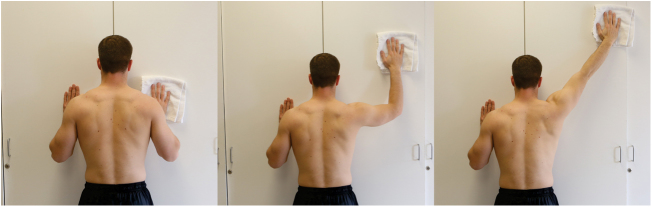
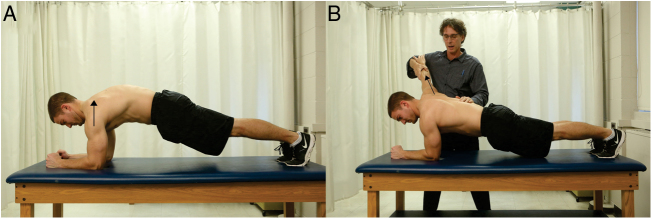
Methods: This paper reviews the anatomy, innervation, testing, and complex actions of the SA. In addition, this paper describes the classic signs and symptoms of weakness or reduced activation of the SA. Several exercises are described and illustrated that purportedly target the activation of the SA, with the intention of optimizing muscular control and encouraging pain free shoulder motion.
Conclusions: This review provides the theoretical background and literature-based evidence that can help explain the SA's complex pathokinesiology, as well as guide the clinician to further develop exercises that likely challenge the muscle. This paper is written along with a companion paper entitled: Kinesiologic considerations for targeting activation of scapulothoracic muscles: part 2: trapezius. Both papers prepare the reader to expand their pallet of exercises that target and challenge these two dominant muscles, with a goal of improving function of the shoulder for several painful conditions caused by their reduced or altered activation pattern.
Keywords: Physical therapy; Scapular dyskinesis; Scapulothoracic joint; Serratus anterior exercises; Shoulder rehabilitation.
Copyright © 2019 Associação Brasileira de Pesquisa e Pós-Graduação em Fisioterapia. Publicado por Elsevier Editora Ltda. All rights reserved.
Figures



References
-
- Neumann D.A. 3rd ed. Elsevier; St Louis: 2017. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation.
-
- Standring S. 41st ed. Elsevier; St Louis: 2016. Gray's Anatomy: The Anatomical Basis of Clinical Practice.
-
- Berthold J.B., Burg T.M., Nussbaum R.P. Long thoracic nerve injury caused by overhead weight lifting leading to scapular dyskinesis and medial scapular winging. J Am Osteopath Assoc. 2017;117(2):133–137. - PubMed
-
- Friedenberg S.M., Zimprich T., Harper C.M. The natural history of long thoracic and spinal accessory neuropathies. Muscle Nerve. 2002;25:535–539. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
