

Iron, Hepcidin, and Death in Human AKI
- PMID: 30737269
- PMCID: PMC6405140
- DOI: 10.1681/ASN.2018100979
Iron, Hepcidin, and Death in Human AKI
Abstract
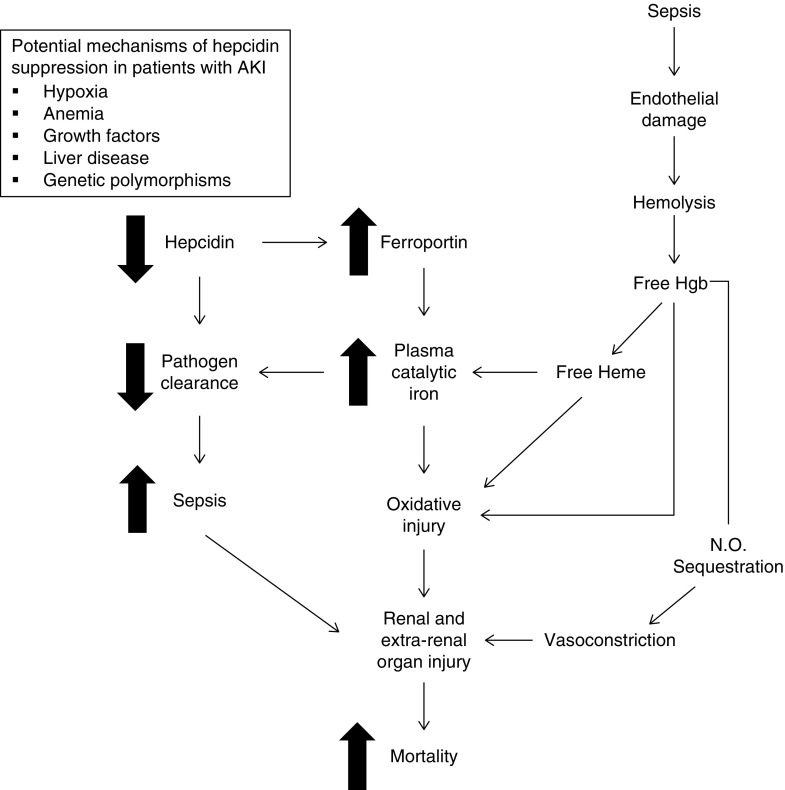
Background: Iron is a key mediator of AKI in animal models, but data on circulating iron parameters in human AKI are limited.
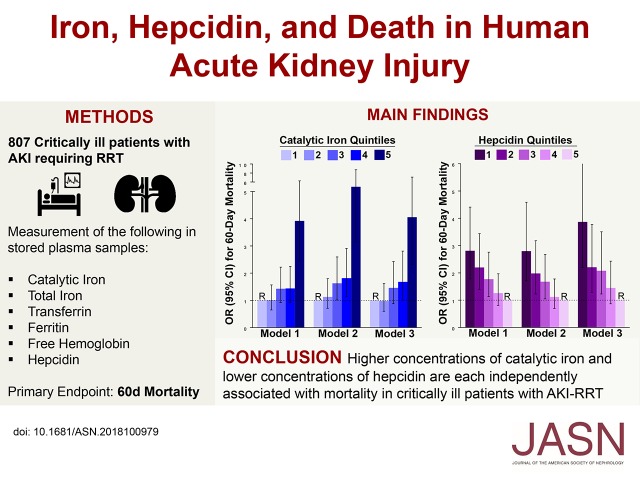
Methods: We examined results from the ARF Trial Network study to assess the association of plasma catalytic iron, total iron, transferrin, ferritin, free hemoglobin, and hepcidin with 60-day mortality. Participants included critically ill patients with AKI requiring RRT who were enrolled in the study.
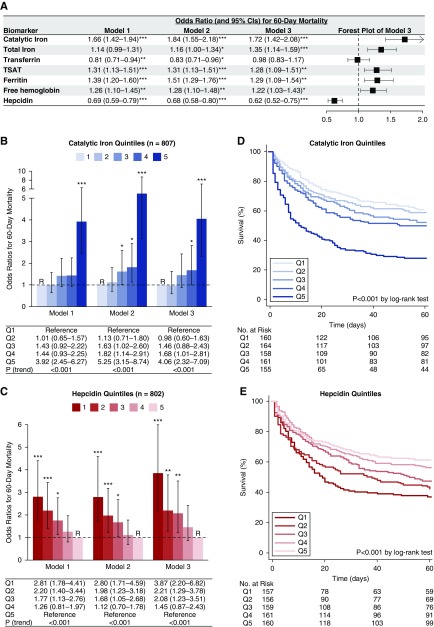
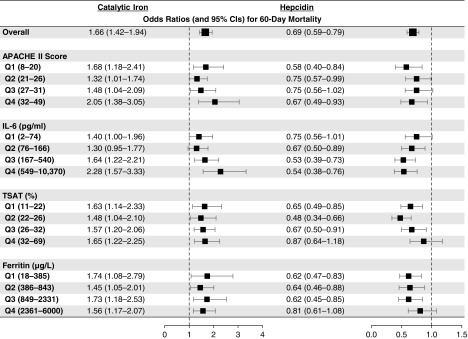
Results: Of the 807 study participants, 409 (51%) died by day 60. In both unadjusted and multivariable adjusted models, higher plasma concentrations of catalytic iron were associated with a significantly greater risk of death, as were lower concentrations of hepcidin. After adjusting for other factors, patients with catalytic iron levels in the highest quintile versus the lowest quintile had a 4.06-fold increased risk of death, and patients with hepcidin levels in the lowest quintile versus the highest quintile of hepcidin had a 3.87-fold increased risk of death. These findings were consistent across multiple subgroups. Other iron markers were also associated with death, but the magnitude of the association was greatest for catalytic iron and hepcidin. Higher plasma concentrations of catalytic iron and lower concentrations of hepcidin are each independently associated with mortality in critically ill patients with AKI requiring RRT.
Conclusions: These findings suggest that plasma concentrations of catalytic iron and hepcidin may be useful prognostic markers in patients with AKI. Studies are needed to determine whether strategies to reduce catalytic iron or increase hepcidin might be beneficial in this patient population.
Keywords: acute renal failure; mortality risk; nephrotoxicity; outcomes.
Copyright © 2019 by the American Society of Nephrology.
Figures

References
-
- Baliga R, Zhang Z, Baliga M, Ueda N, Shah SV: In vitro and in vivo evidence suggesting a role for iron in cisplatin-induced nephrotoxicity. Kidney Int 53: 394–401, 1998 - PubMed
-
- Baliga R, Zhang Z, Baliga M, Shah SV: Evidence for cytochrome P-450 as a source of catalytic iron in myoglobinuric acute renal failure. Kidney Int 49: 362–369, 1996 - PubMed
-
- Paller MS: Hemoglobin- and myoglobin-induced acute renal failure in rats: Role of iron in nephrotoxicity. Am J Physiol 255: F539–F544, 1988 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
